
Case contribution: Dr Radhiana Hassan
Clinical:
- A 55 years old lady
- Underlying pancytopenia, unknown cause as patient refused BMAT and defaulted follow up.
- Newly diagnosed left breast cancer T3N1Mo, Initially planned for mastectomy and axillary clearance but noted pancytopenia (Hb=8.0, WBC=1.4 and Plt 44) and admitted for further investigations.
- CT scan was done as part of tumour staging
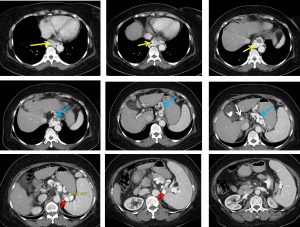
CT scan findings:
- Serpiginous dilated vessels are detected at gastroesophageal junction around the distal oesophagus (yellow arrows) , gastric (yellow arrows) and perisplenic region(red arrows).
- Filling defect is identified within the main portal vein and extending to the right and left portal vein branches. However, the distal portal vein branches are still opacified. The portal vein is still normal in calibre measuring 1.0 cm
- Liver is normal in size. Liver margin is slightly nodular. No lesion is seen within the liver. No intrahepatic ductal dilatation is noted.
- Gallbladder wall is thickened with pericholecystic fluid observed. Multiple stone is seen within the gallbladder. Common bile duct is normal in calibre.
- Spleen is enlarged measuring 15.4 cm in largest span.
- No free fluid within the abdomen.
Diagnosis: Portal vein thrombosis with portosytemic collateral varices
Discussion:
- Portal hypertension is common clinical syndrome defined as increase in portal venous pressure. This results in rerouting of blood flow away from the liver through the collateral pathways to low pressure systemic veins.
- Normal portal venous pressure is between 5-10 mmHg. Pathological increase in PVP is primarily caused by resistance to portal inflow and could be due to many conditions. Ongoing portal hypertension eventually leads to formation of collateral circulations that directly connects the portal blood vessels to systemic circulation bypassing the liver.
- These portosytemic circulations include coronary (left gastric) veins, esophageal, paraesophageal, cardiophrenic , gastric, perisplenic, splenorenal and splenocaval varices.
- Coronary (left gastric) veins- within the lesser omentum are most frequently depicted varices. A coronary vein larger than 5-6 mm on CT scan is considered abnormal. It is usually accompanied with esophageal or paraesophageal varices.
- Esophageal varices-the most common and important collateral vessels in the wall of the lower esophagus.
- Paraesophageal varices-venous collaterals surrounding the esophagus and connect the coronary vein with azygous, hemiazygous and the vertebral plexus, seen as dilated vessels surrounding the esophagus and descending thoracic aorta.
- Cardiophrenic angle varices-dilated percardiophrenic veins seen as undulating masses along the cardiac border.
- Gastric varices –along with esophageal varices are the most common pathways seen in portal hypertension
- Perisplenic varices- dilated veins in the anteroinferior aspect of spleen.
- Others include paraumbilical and abdominal wall and mesenteric collaterals
Recent Comments