
Case contribution: Dr Radhiana Hassan
Clinical:
- A 34 years old man
- No known medical illness
- Presented with left neck swelling for 2 years
- Not painful, not causing any compressive symptoms
- No loss of appetite or loss of weight
CT scan findings:
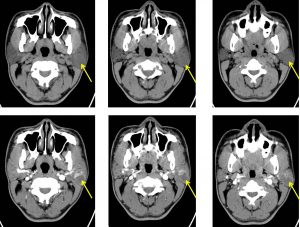
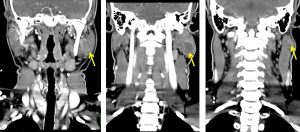
- The left parotid gland is bulky.
- A rounded well-defined hypodense (HU 30 – 45) lesion is seen at the superficial lobe of left parotid gland, measures about 2.0 cm x 2.3 cm x 2.4 cm (AP x W x CC).
- In post contrast images, the lesion is hypodense compared to the normally enhancing parotid tissue. The lesion itself shows wall enhancement.
- No necrotic region or calcification within the lesion.
- The deep lobe of left parotid gland shows normal parenchymal enhancement.
- No significant mass effect to the surrounding structures.
- No infiltration to the adjacent sternocleidomastoid muscle.
- Left internal jugular vein and left internal carotid artery are patent.
- Multiple shotty cervical lymph nodes.
HPE findings:
- Macroscopy: specimen labelled as left parotid gland consist of three pieces of whitish tissue. Cut section shows whitish surface. No area of hemorrhage or necrosis seen.
- Microscopy: Sections from the pieces show well-circumscribed and encapsulated tumor composed of epithelial elements dispersed within mesenchymal-like background of loose myxoid connective tissue. The epithelial elements form gland, strands and sheets of cells. Island of squamous epithelium with keratinisation are also seen. There is no necrosis or mitotic figure noted.
- Interpretation: Pleomorphic adenoma.
Diagnosis: Pleomorphic adenoma of parotid gland.
Discussion:
- Pleomorphic adenomas also known as benign mixed tumours.
- It is the most common salivary gland tumours.
- Involvement of parotid>submandibular>minor salivary gland>sublingual gland.
- Typically seen in middle aged, slightly higher incidence in females than males.
- Pathologically composed of a mixture of variable histology. Three types has been described; myxoid, cellular and classic.
- On imaging, it is typically seen as rounded mass with well-defined lobulated borders within the parotid gland particularly the superficial lobe. On ultrasound it is typically hypoechoic and may show posterior acoustic enhancement. CT scan shows homogenous density with prominent enhancement. However, larger mass can show heterogenous, less enhancement with foci of necrosis and even delayed enhancement. Small calcifications are common. The lesion is typically hypovascular on angiongram. MRI shows T1 hypointensity, Ty hyperintensity with homogenous enhancement.
- There is a small risk of malignant transformation.
Recent Comments