
Case contribution: Dr Radhiana Hassan
Clinical:
- An 82 years old lady
- UnderlyingDM, HPT, hyperlipidaemia,
- Presented with incoherent speech and lower limb weakness.
- Clinical examination shows GCS E4V4M6, power lower limbs 3/5.
- Fluctuation in GCS is due to metabolic disorders (acute CKD with urea 23 and metabolic acidosis)
- Improve during hospitalization
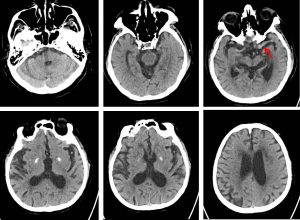
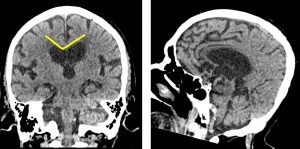
CT scan findings:
- There is dilatation of lateral, third and fourth ventricles
- Widening of CSF spaces seen, more prominent at frontotemporal region.
- No crowding of vertex. Callosal angle is normal.
- Left MCA appears dilated (red arrow)
- A few areas of lacunar infarctions are also seen
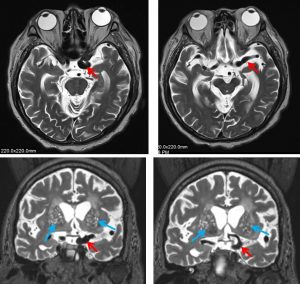
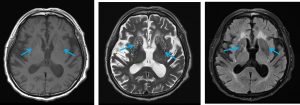
MRI findings:
- MRI better demonstrate the fusiform dilatation of left distal ICA extending to MCA (red arrows)
- No saccular aneurysm is seen
- The are numerous T1-hypointense, T2-hyperintense and FLAIR suppressed lesions in both basal ganglia with almost symmetrical distributions (blue arrows). This is in keeping with dilated perivascular spaces.
- No acute infarction seen
- Generalised cerebral atrophy with leukoariosis are also seen
Diagnosis: Fusiform MCA aneurysm with dilated perivascular space and cerebral atrophy
Discussion:
- Dilated perivascular spaces (PVS) is seen as cluster of variable-sized fluid-filled spaces similar to CSF signal intensity
- Most common site for PVS is basal ganglia.
- Other location includes midbrain, deep white matter, subinsular cortex, thalami and corpus callosum, dentate nuclei
- Fusiform aneurysm of intracranial vessels are usually caused by atherosclerotic disease. It comprises 3-13% of intracranial aneurysms. Most cases are treated conservatively.
Recent Comments