
Case contribution: Dr Radhiana Hassan
Clinical:
- A 60 years old lady
- No known medical illness
- Presented with abdominal pain x 3/7, initially generalised then radiated to right iliac fossa region
- Associated with vomiting and loss of appetite.
- No fever, no altered bowel motion, no UTI or URTI symptoms
- Clinical examination shows mild tenderness at RIF with vague mass. TWBC=18, renal profile normal, liver function test is also normal

X-ray findings:
- Multiple calcified foci are seen projected over the right hypochondriac region likely gallstones (yellow arrow)
- A few opacities are also seen within the left pelvic cavity (white arrow)
- No dilated bowel loops or pneumoperitoneum.

Ultrasound abdomen findings:
- Liver is not enlarged and shows homogeneous parenchymal echogenicity with no focal lesion within it.
- The gall bladder is well distended and shows multiple calculi within its lumen. The wall is not thickened and no pericholecystic collection is observed.
- Intrahepatic and extrahepatic ducts are not dilated.
- No pelvic mass seen. No collection in RIF seen. There is no free fluid.
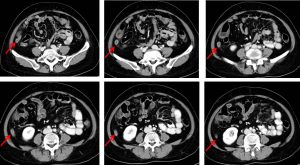
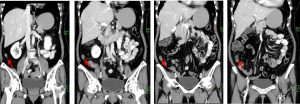
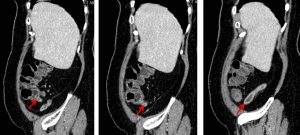
CT scan findings:
- A blind end tubular structure that is continuous with caecum is identified at retrocaecal region, representing an appendix (red arrows).
- It appears dilated and fluid filled, the maximal transverse external diameter measures about 1.1cm at its body.
- Mucosal wall enhancement is noted, however appears intact with no apparent area of discontinuity.
- Minimal periappendiceal fat streakiness. No surrounding fluid or collection is detected. No pneumoperitoneum.
- No evidence of appendicolith. No dilated bowel.
- Cholelithiasis is as noted on ultrasound with no evidence of active infection.
- Uterine fibroids with intralesional calcifications.
Diagnosis: Acute appendicitis with no evidence of perforation.
Discussion:
- Appendicitis remains the most common acute surgical condition of the abdomen
- Accurate and timely diagnosis of acute appendicitis is essential to minimize morbidity.
- The case-fatality rate of appendicitis jumps from less than1 percent in nonperforated cases to 5 percent or higher when perforation occurs
- The diagnosis of appendicitis traditionally has been based on clinical features found primarily in the patient’s history and physical examination
- Atypical presentations can result in delays in treatment, unnecessary hospital admissions for observation, and unnecessary surgery.
- Imagings have been shown to increase diagnostic accuracy and patient outcomes in these cases
- Diagnostic accuracy of ultrasound ranges from 71-97%.
- Diagnostic accuracy of CT scan ranges from 93-98%.
Recent Comments