
Case contribution: Dr Radhiana Hassan
Clinical:
- A 41 years old man with underlying DM, HPT and dyslipidaemia
- Presented with right hypochondriac pain for 4 days
- Associated with fever for one week
- Also had nausea and reduced oral intake.
- Condition worsened and admitted for 5 days in ICU due to sepsis.
- Blood culture: Burkholderia pseudomallei, HBA1C=13.4%

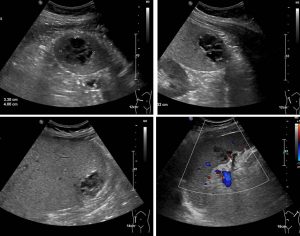
Ultrasound findings:
- The liver has normal parenchyma echogenicity. It has smooth margin. Liver is enlarged measuring approximately 18 cm at midclavicular line.
- There is a hypoechoic lesion with ill-defined margin seen at segment VI measuring 3.3 x 4.0 x 4.3 cm (AP x W x CC). This lesion has internal septations and echogenic debris within.
- Spleen is enlarged measuring 14.0 cm. There is a hypoechoic lesion with ill-defined margin adjacent to the hilum measuring approximately 2.0 x 3.1 cm (AP x W). This lesion has internal septations and echogenic debris within.
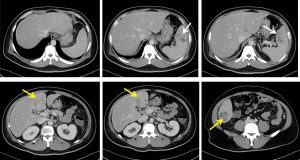
CT scan findings:
- Liver is enlarged measuring about 25 cm in craniocaudal length. It shows fatty change.
- Two peripherally enhancing ill-defined multiloculated lesions with central low attenuation are identified in segment VI and IV (yellow arrows). They are measuring 3.9 x 3.3 x 3.2 cm and 2.8 x 3.5 x 2.2 cm (AP x W x CC) respectively suggestive of abscesses.
- The gallbladder is distended with thickened enhancing wall and pericholecystic fluid collection. No layering density within. No gallbladder calculus. Gallbladder wall is intact.
- Ill-defined multiloculated non-enhancing hypodense lesion is also seen in the upper pole of the spleen measuring 3.6 x 1.8 x 2.3 cm (AP x W x CC). Reactive fluid is seen medially adjacent to this collection in the splenic hilum.
- The splenic hilar vessels are grossly patent and not thrombosed.
Diagnosis: Meliodosis with spleen and liver abscesses.
Discussion:
- Meliodosis is a bacterial infection caused by Burkolderia pseudomallei
- It is most commonly infects adult with underlying predisposing factors mainly diabetes mellitus.
- Spleen is the most commonly affected extrapulmonary visceral organ.
- Splenic lesions are often multiple, small and discrete varying from 0.5 cm to 1.5 cm, single or multiloculated lesions, subcapsular collections with or without peripslenic extension.
- Concurrent spleen and liver abscesses are more likely to be associated with meliodosis than with infections with other organisms.
- Liver is the second most common visceral organ affected by meliodosis. Similar with splenic lesion, appearance on imaging may varies. Liver involvement is usually part of multi-organ involvement rather than a solitary organ involvement.
- Other organs to be involved: kidneys and prostate
- Rare involvement: bowel and peritoneum causing enteritis, colitis and peritonitis
Progress of patient:
- Completed IV meropenem followed by Bactrim.
- Patient responded and discharged well.
- A repeat CT scan 3 months later shows resolution of abscesses foci.
Recent Comments