
Case contribution: Dr Radhiana Hassan
Clinical:
- A 67 years old man
- Had underlying bronchial asthma
- History of appendicectomy at 11 years old
- Presented with abdominal pain for 3 days, generalised and colicky in nature. Pain score 4-5.
- Associated with abdominal distension, NBO and not passing flatus. NO PR bleed.
- Had history of loss of appetite and loss of weight for 1 month
- Father had liver cancer, no other malignancy in family
- Clinical examination shows distended abdomen, generalized voluntary guarding, tingling bowel sound, no mass palpable. No abnormal lymph node.
- Rectal examination shows hypertrophic anal papillae, empty rectum, enlarged prostate with no other mass lesion.
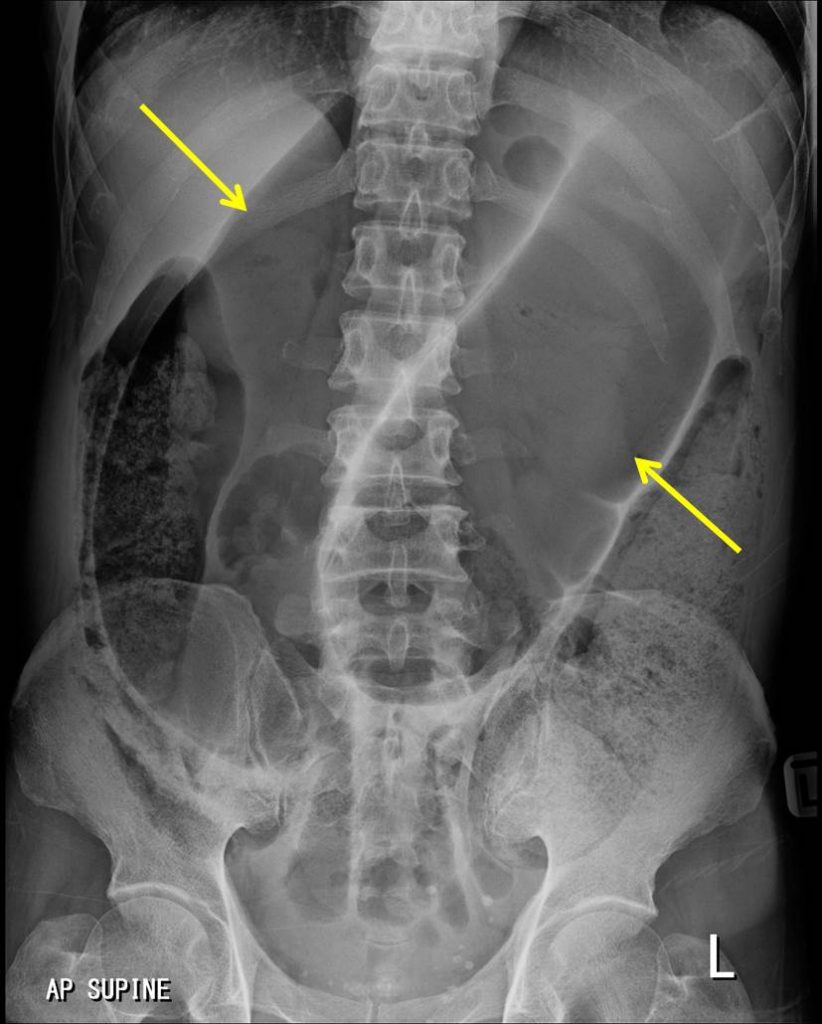
Abdominal radiograph findings:
- Dilated bowel loops, no haustration
- It demonstrate coffee-bean sign
- No free intraperitoneal air is seen
- Abundance fecal material in colon
Intraoperative findings:
- Gangrenous dilated sigmoid colon
- No perforation, no fecal contamination
- Hemorrhagic fluid upon entering the peritoneum
- Dilated descending and transverse colon
- Normal caecum, small bowel, stomach, gallbladder and liver
- EBL= 100 ml.
- Sigmoid colectomy and hartmann procedure performed
Diagnosis: Sigmoid volvulus
Discussion:
- Sigmoid volvulus is the most common GI tract volvulus
- It accounts for about 8% of all intestinal obstructions
- Patient almost always have history of constipation.
- It has a high mortality rate of 20-25%
- Peak age >50 years old
- Abdominal plain film is usually diagnostic. It shows inverted U-shaped distended sigmoid loop, loss of haustra
- A coffee-bean sign is a well-known sign showing a midline crease corresponding to mesenteric root in a greatly distended sigmoid
- The distended loop points towards the right upper quadrant as compared to caecal volvulus which usually pointing to left upper quadrant
Recent Comments