
Case contribution: Dr Radhiana Hassan
Clinical:
- a 12 years old girl
- Presented with bilateral eye proptosis, gradual in severity over one year
- Clinical examination shows small build girl with abnormal body figure
- Bilateral proptosis with normal extraocular muscle movement
- Visual acuity of both eyes are 6/6.
- Cranial nerves are intact
MRI brain and orbit findings:
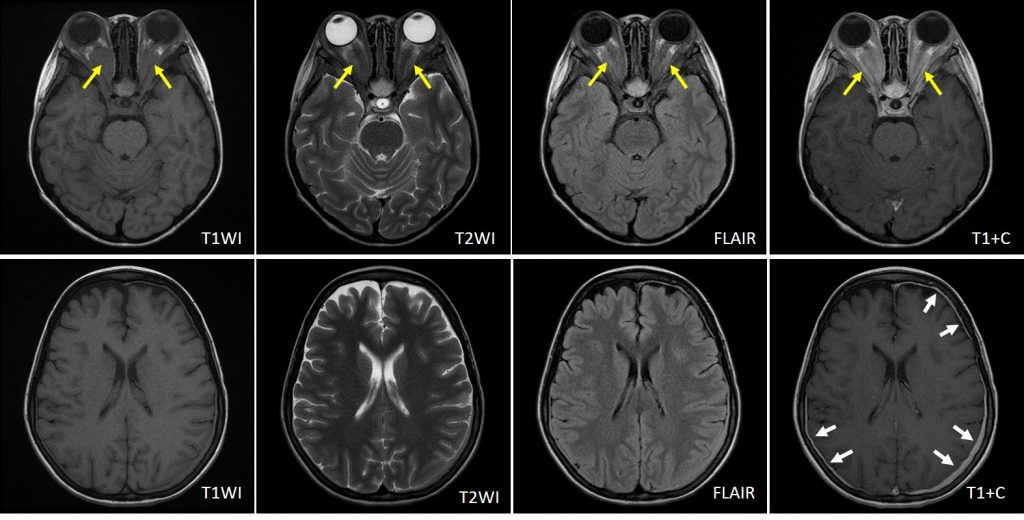
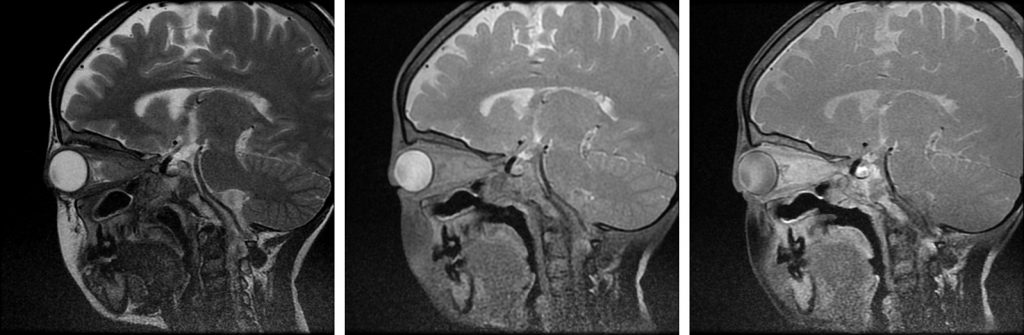
- There are bilateral intraconal soft tissue mass (yellow arrows) which is isointense to muscle on T1 and T2WI with homogenous enhancement post contrast. It is not suppressed on STIR sequence.
- The lesion is causing bilateral proptosis.
- Optic nerve is seen encased within the lesion but no obvious infiltration. Both optic nerves look prominent with normal signal intensity
- Posterior extension to orbital apex but no expansion or widening of the canal
- No abnormal enhancement of the optic chiasm.
- Globes and extra-ocular muscles are normal.
- Pituitary gland is also normal (images not shown)
- Smooth dural thickening (white arrows) are also seen
Diagnosis: Erdheim-Chester Disease (presumed diagnosis)
Progress:
- Patient was referred to another centre for tissue biopsy and genetic work up
Discussion:
- Erdheim-Chester disease is a rare non-Langerhans cell, non-familial multisystemic histiocytosis with widespread manifestation of highly variable severity.
- In contrast to Langerhans cell histiocytosis (LCH), no S-100 nor CD1 are detected but CD68 is positive.
- Both Erdheim-Chester and LCH may coexist.
- It is a rare disease with a slight male predominance.
- Patient presented with a variety of symptoms depending on organ involvement.
- Musculoskeletal involvement is the most common.
- Visceral involvement include lung, kidneys, retroperitoneum, heart, pericardium, aorta, skin and retro-orbital tissue.
- Neurological manifestation include exophthalmos and diabetes insipidus from pituitary involvement (infundibulum and hypothalamus).
- Retro- orbital changes include optic nerve oedema, retrobulbar mass that cause proptosis and motility impairment, retrograde extension along the optic nerve to the hypothalamus with brain involvement.
- Intracranial involvement of the dura, brain and pituitary are rare. Dural involvement may mimics meningioma
Recent Comments