
Case contribution: Dr Nurul Akhmar Omar
Clinical:
- A 6 weeks old baby, born premature at 34 weeks
- Noted tachypnoiec at birth and treated as congenital pneumonia
- Presented again at 3 weeks old with respiratory distress. Persistent tachypnoe and need oxygen.
![]()
Chest radiograph findings:
- An area of lucency is seen in the left mid and lower zones (yellow arrows).
- Paucity of bronchopulmonary markings within the lucent region.
- No obliteration of left hemidiaphragm.
- Mediastinal shift to the right side (white arrow).
- Trachea and the bronchi shadows are normal.
- Nasogastric tube is seen in-situ.
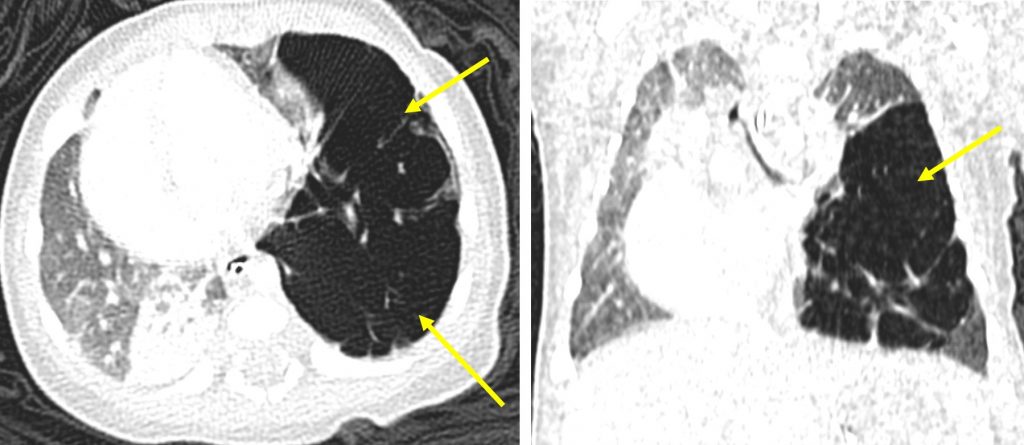
CT scan findings:
- The hyperinflated left lower lobe is confirmed
- There is associated mediastinal shift to the right,
- The left upper lobe is compressed
- Segmental collapse consolidation of right lower lobe is also seen.
- Bronchial tree is normal.
Diagnosis: Congenital lobar overinflation (CLO)
Discussion:
- CLO is previously known as congenital lobar emphysema (CLE).
- It is a congenital abnormality resulting in progressive overinflation of one or more lobules of a neonate’s lung.
- It is more common in males.
- Associations include: aberrant left pulmonary artery, VSD, PDA and tetralogy of Fallot.
- Radiographic features:
- During iImmediate postpartum period, the affected lobe tends to appear opaque and homogenous
- Later findings include areas of hyperlucency in the lung with oligaemia (i.e paucity of vessels), mass effect with mediastinal shift and hemidiaphragmatic depression. A lateral view may show posterior displacement of the heart.
- CT scan usually confirms the diagnosis and show greater detail of the mediastinal vascular structures, compressive atelectasis of adjacent lobes and attenuation of vascular structures in affected lobe.
- Treatment depends on clinical symptoms. Patient with mild symptom is followed up. Those with severe symptoms may need surgical resection or lobectomy.
Recent Comments