
Case contribution: Dr Radhiana Hassan
Clinical:
- A 20 years old male, presented with neck pain for 4 months which is partially relieved with pain killers
- No history of trauma or fall prior to onset of pain
- No associated upper limb weakness, no constitutional symptoms, no contact with PTB patient
- Clinically no neck tenderness and no neurological deficit
- Blood investigations normal
- AFB and Mantoux test are also normal
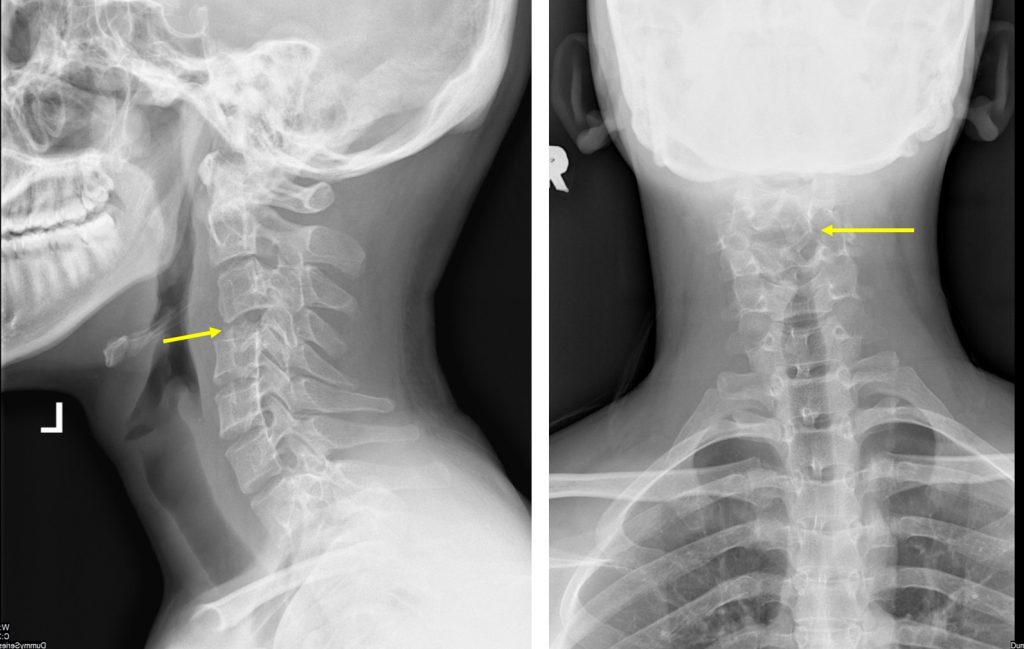
Cervical spine radiograph in AP and lateral views:
- Flattening of C4 vertebral body (yellow arrows)
- The posterior element is preserved
- Minimal retrolisthesis of C3 over C5 vertebral body
- Intervertebral disc spaces are preserved
- Pedicles of visualized vertebrae are intact
- No prevertebral soft tissue swelling
- No abnormal air pockets within the soft tissue
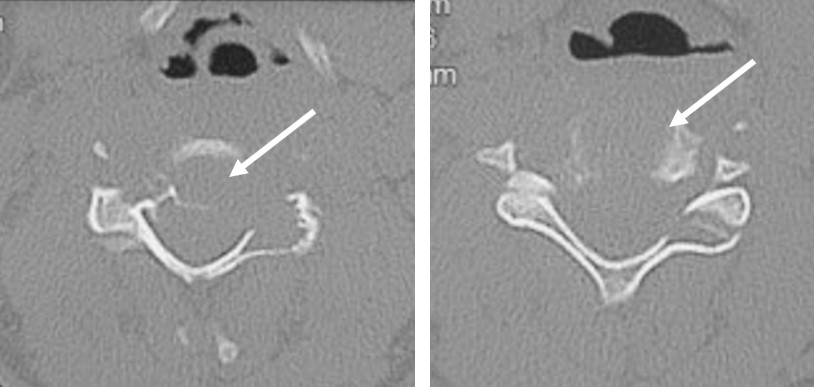
CT scan in axial planes bone window confirms lytic destruction of C4 vertebral body. Lytic destruction is also seen involving the lamina and pedicles bilaterally.

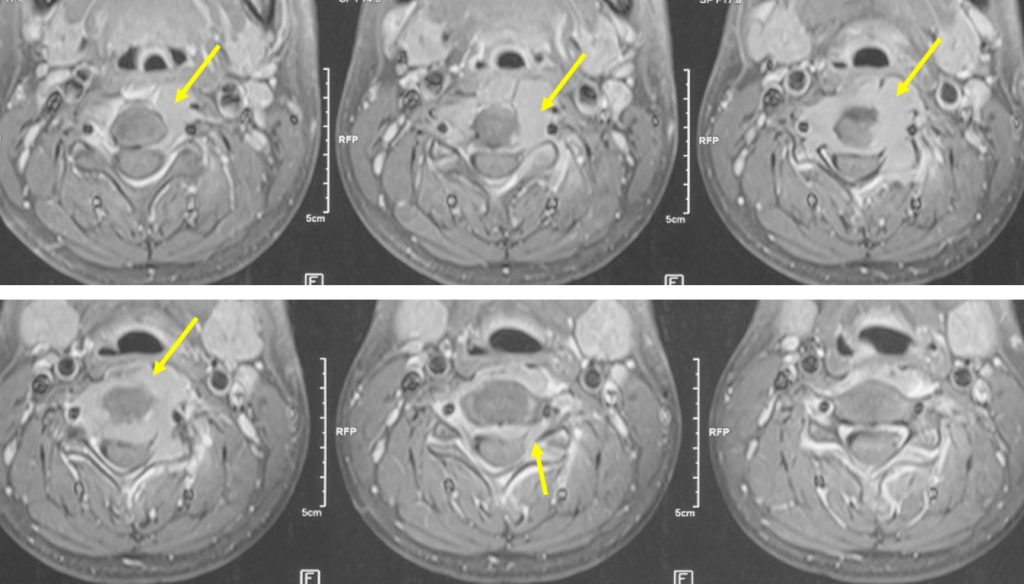
MRI of cervical spine in sagittal T2 and axial T1 post contrast:
- Destruction of C4 is seen with associated surrounding soft tissue
- Upper and lower intervertebral disc spaces are preserved
- Soft tissue mass extension into spinal canal causing compression of cord
- No abnormal signal intensity within the cord
HPE findings:
- Macroscopy: specimen labelled as tumour and bone from C4 consists of multiple pieces of brownish tissues
- Microscopy: sections show fragments of lesional tissue displaying numerous osteoclastic multinucleated giant cells with mononuclear stroma cells in the background. The mononuclear cells are uniform. There is no nuclear atypia or increase in mitosis seen. No epitheliod granuloma seen.
- Impression: Suggestive of giant cell tumour
Diagnosis: Giant cell tumour (GCT) of cervical spine
Discussion:
- Giant cell tumour (GCT) is a benign primary bone tumour that has a locally aggressive behaviour. It rarely undergoes malignant transformation.
- It is most frequently seen at metaphyseal/epiphyseal region of the long bones. It affect spine in 2-7% of cases. It is rarely found in the cervical spine.
- The presence of osteolysis and trabeculations in imaging studies are suggestive of GCT, but the definitive diagnosis requires histopathology result.
- Magnetic resonance imaging has the best sensitivity for detecting extent of soft tissue, cystic components and fluid-fluid levels.
- The treatment is mainly surgical, in the attempt to resect the entire lesion whenever possible, especially if there may be neurological involvement
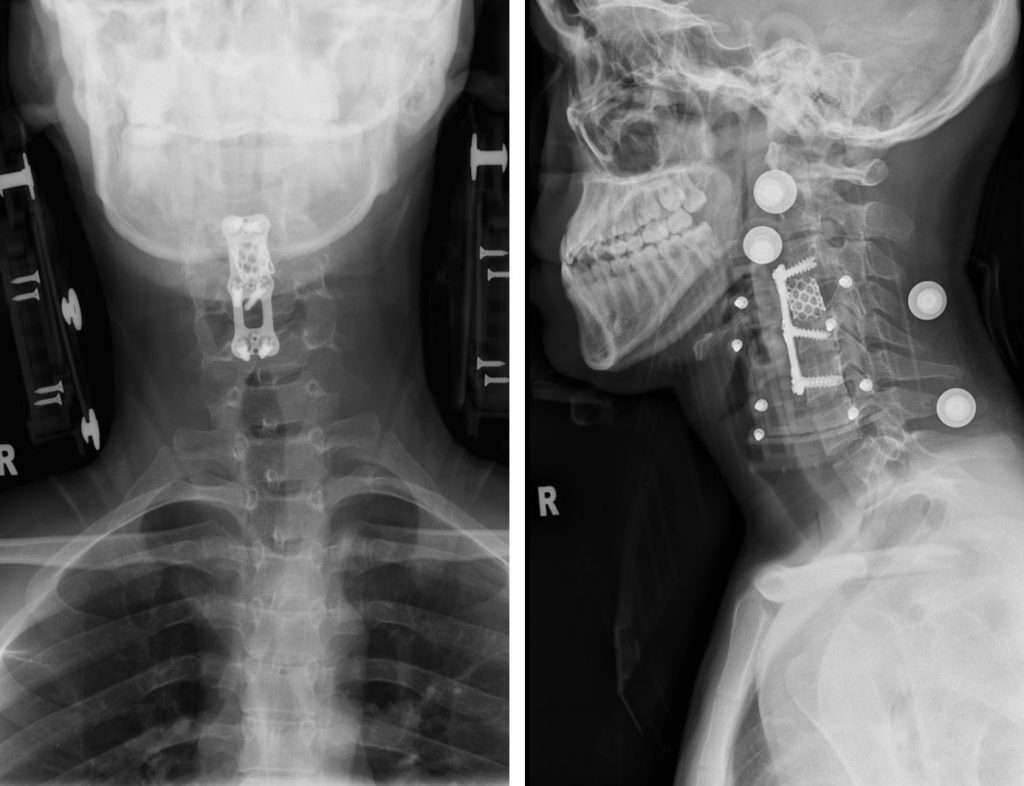
Progress of patient:
- Anterior cervical corpectomy and fusion done under GA
- Subsequent CT thorax, abdomen and pelvis done shows no other bone lesion. No evidence of metastasis.
- Patient was discharged well
Recent Comments