
Case contribution: Dr Radhiana Hassan
Clinical:
- A 44 years old with epigastric pain
- CXR requested to rule out perforated peptic ulcer disease

Radiographic findings:
- Right hemidiaphragm is significantly higher than the left side
- The difference between dome height is more than 3 cm
- Blunting of right costophrenic angle with meniscus sign
- No free air under the diaphragm
- Lungs are clear
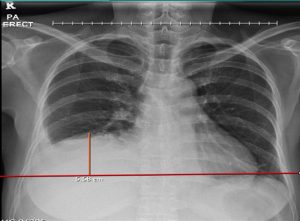
Impression: Elevated right hemidiaphragm
Discussion:
Normal radiographic anatomy of diaphragm:
- Both diagram contours should be visible medially to the spine
- Both diaphragm should form a sharp margin with lateral chest wall
- During inspiration, the top of right diaphragmatic dome coincides with the end of anterior 5th or 6th rib
- It can be slightly higher in obese, the elderly and young infants
- In over 90% of normal people the right hemidiaphragm is higher than the left
- The left hemidiaphragm is usually 1.5 -3.0 cm lower than the right due to heart’s weight
- In about 10% of population the left hemidiaphragm is at the same level or higher than the right.
Causes of elevated hemidiaphragm
- Above the diaphragm
- Decreased lung volume: atelectasis, collapsed, prior lobectomy or pneumonectomy, pulmonary hypoplasia
- Pneumonia or pleuritic pain
- Diaphragm
- Phrenic nerve palsy, diaphragmatic eventration, contralateral stroke
- Below the diaphragm
- Abdominal tumour such as liver metastasis or primary liver disease
- Subphrenic abscess
- Distended stomach or colon including Chilaiditi syndrome
- Others
- Dorsal scoliosis
- Ribs fracture
Progress of patient:
- Ultrasound showed enlarged liver with multiple lesions within the liver parenchyma
- Subsequent investigations revealed metastatic liver disease secondary from GI malignancy

Recent Comments