
Case contribution: Dr Radhiana Hassan
Clinical:
- A 47 years old lady
- Para 2, last child birth 16 years ago
- Presented with progressive abdominal distention for 3 months
- Gradually increased in size
- Per abdomen shows mass about 28 weeks size
- Ultrasound shows huge multiloculated ovarian lesion
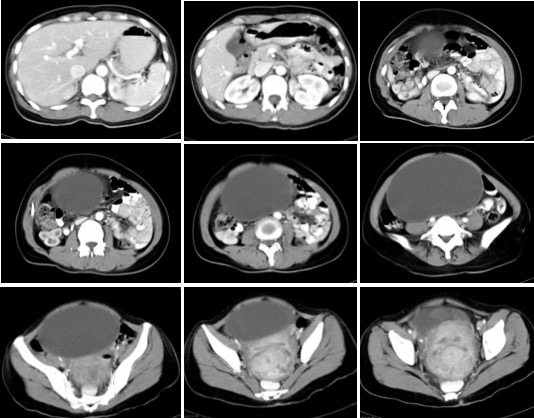
CT scan findings:
- A large well-defined mass in the abdomen measuring about 17x10x20 cm.
- The density is homogenous and consistent with cyst
- No calcification or solid component within.
- There is thin septation seen at the right side of the mass.
- The bowels are displaced laterally.
- The uterus is enlarged with multiple lesions within the myometrium.
- Liver, spleen, pancreas, both adrenal glands and kidneys are normal.
- No lymphadenopathies. No ascites.
Intra-operative findings:
- Left ovarian tumour, cystic with thin wall, benign-looking, 15×15 cm
- Right ovary normal
- Minimal peritoneal fluid, omentum normal
- No peritoneal deposit, liver surface smooth
Histopathological findings:
- Macroscopy: The whole specimen labelled as ovarian tumour, both fallopian tubes, both ovaries, cervix and uterus weighs 2100 gms. The uterus measures 80 mm from cornu to cornu, 120 mm from fundus to cervix and 70 mm in antero-posterior diameter. The left ovarian cyst measures 180x150x90 mm. The external surface of the cyst is smooth and the capsule intact. Cut section of uterus shows multiple well-defined tumour in the anterior and posterior uterine wall. The tumour has whitish cut surface with whorl appearance. Cut section of the ovarian cyst show a multiloculated cyst with one huge locule and multiple small locules at one area. The cyst contain clear, watery serous fluid. The wall of the cyst measures 1-2 mm in thickness.
- Microscopy: The endometrium is non-secretory. Multiple benign tumours are seen in the myometrium consists of spindle nuclei with blunt-ended end without nuclear atypia, arranged as fascicles and as intersecting bundles. Mitosis is not seen. The left ovarian cyst wall is lined by flattened cuboidal epithelium with occasional ciliated cells. No evidence of malignancy seen.
Diagnosis: Left ovarian cyst: serous cystadenoma. Uterus: leiomyoma
Discussion: Serous cystadenoma of the ovary
- A benign ovarian epithelial tumour
- the commonest type of ovarian epithelial tumours
- peak incidence at 4th to 5th decades of life
- Generally asymptomatic. If symptoms are present, they are usually related to mass effect with displacement of adjacent structures
- They can be bilateral in ~15% of cases.
- CT scan often seen as a unilocular (typically) or multilocular cystic mass with homogeneous CT attenuation, with a thin regular wall or septum, and usually no endocystic or exocystic vegetation.
- Cysts can be quite large in size and have the potential to be seen filling most of the lower pelvis with extension into the upper abdomen.
- Unilocular cystic masses in the adnexal region are more likely benign and can have both non-ovarian or ovarian origin. Paraovarian cysts, hydrosalpinx, pyosalpinx and hematosalpinx are the most common extraovarian lesions, whereas ovarian lesions are usually represented by functional cysts and serous cystadenomas
Recent Comments