
Clinical:
- A 55 years old man with DM, HPT and CVA 4 years ago
- Presented with acute onset of aggressive behaviour.
- Also noted serum HSV IgG +ve, CSF protein 716.
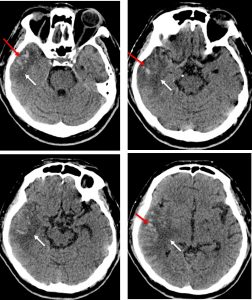
CT scan findings:
- An area of hypodensity at right temporal region (white arrows)
- Minimal effacement of the sulci at the same area
- Multifoci hyperdensities are also seen within (red arrows)
- No mass effect or midline shift
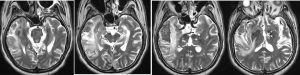
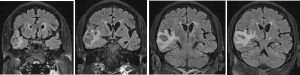

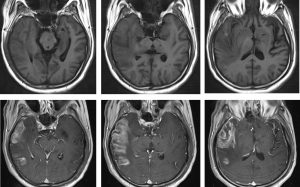
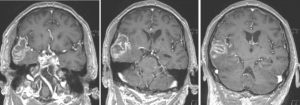
MRI findings:
- Hyperintense areas on both T2 and Flair affecting the right temporal lobe (both the grey and white matter). This area appears wedge shaped (on coronal Flair) and is confined within the MCA territory.
- Involvement of the right insular cortex noted.
- The hippocampus/medial temporal, the inferior aspect of the right temporal lobe and frontal lobes are not affected.
- Associated areas of acute haemorrhage within.
- Presence of gyriform enhancement noted in the affected brain.
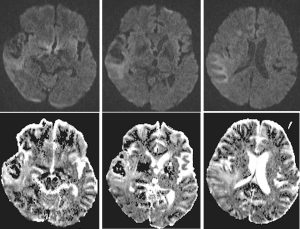
- No significant fluid restriction on DWI.
- Multiple old lacunar infarcts in both thalami and left corona radiata with underlying small vessel ischaemia changes.
- No definite abnormal leptomeningeal enhancement.
- Interpretation: Overall features are more consistent of haemorrhagic subacute infarct in the right MCA territory in the right temporal lobe than herpes encephalitis.
Progress of patient:
- Patient was treated as HSV encephalitis and completed Aciclovir 2/52
- A repeat MRI done one month later to reassess condition
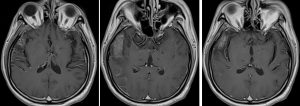
MRI findings:
- The previously seen hyperintense area in the right temporal lobe show involutional changes and is still territorial within the MCA territory . The area of gyriform enhancement is smaller.
- There is now volume loss seen. No significant change in the area of intraparenchymal bleeding.
- The signal characteristics of this lesion remains similar, with no diffusion restriction on DWI.
- The hippocampus/medial temporal, the inferior aspect of the right temporal lobe and frontal lobes remains unaffected.
- Multiple old lacunar infarcts in both thalami and left corona radiata are similar.
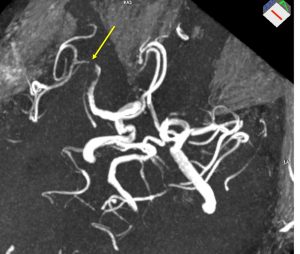
- MRA shows stenotic segments involving junction between M1 and M2 segments of right MCA. No aneurysmal dilatation of the visualised intracranial vessels.
- Interpretation: Repeat MRI shows the brain changes are non progressive and showing involutional changes/volume loss. These changes are suggestive of infarction.
Final diagnosis: Right MCA territorial infarction
Discussion:
- Herpes simplex viral encephalitis (HSVE) is the most frequent cause of sporadic fatal encephalitis in the Western world.
- Nevertheless, the condition is rare and presents with non-specific symptoms; making a diagnosis is challenging.
- Differentiation between HSV and acute infarction can be difficult at times.
- In this cases, MRI features are suggestive of infarction rather than HSV encephalitis
- unilateral involvement; HSV encephalitis has a high affinity for limbic systems with bilateral asymmetrical involvement.
- The basal ganglia are typically spared in HSV encephalitis
- MRA shows the abnormal vessels supporting the infarcted region
- Volume loss on subsequent imaging
Recent Comments