
Clinical:
- A 53 years old man
- Underlying DM and HPT
- Non-functioning left kidney with ESRF on regular hemodialysis
- History of right lower ureteric calculus, open ureteric vesicolithotomy done 2 years ago. After that developed recurrent anterior abdominal abscess
- Current presentation with fever, abdominal pain and pus discharge from anterior abdominal wall
Imaging findings:
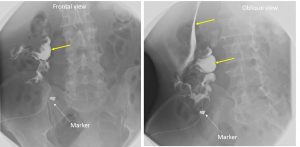
- Fistulogram followed by CT scan abdomen
- Foley’s catheter inserted into anterior abdominal wall ulcer at right iliac fossa region. Low osmolar contrast media, 50 mls in total infused via the catheter.
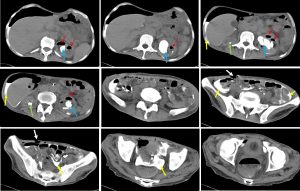
- The contrast is seen in the peritoneal space outlining the bowel loops and the liver with extension into pelvic region (yellow arrows).
- No extension of contrast into lumen of bowel is seen.
- The ureter and urinary bladder is not opacified.
- CT scan shows a shrunken right kidney with multiple calculi within it (green arrows). Left kidney is enlarged with a large staghorn calculus within it (blue arrows). There are low density foci with multiple air pockets seen within the left kidney (red arrows). There is no extrarenal extension or air pockets.
Diagnosis: Peritoneo-cutaneous fistula with emphysematous pyelonephritis of left kidney
Discussion:
- Peritoneocutaneous fistula is defined as communication of the peritoneal cavity with the skin. Previously reported peritoneocutaneous fistula include those due to skin excoriation after large chronic incisional hernia and due to spilled gall stones following laparoscopic cholecystectomy
- Emphysematous pyelonephritis refers to a morbid infection with gas formation within or around the kidneys.
- CT is the best diagnostic modality for emphysematous pyelonephritis, and it may show the following diagnostic features: enlarged, destroyed renal parenchyma, small bubbly or linear streaks of gas, fluid collections, with gas-fluid levels or focal necrotic areas with or without abscess formation.
- In this patient, these two condition co-exist and with underlying DM and ESRF carries high morbidity and mortality risks.
Recent Comments