
Case contribution: Dr Radhiana Hassan
Clinical:
- 57 years old man,
- Underlying DM
- Presented with persistent abdominal pain.
- Clinically tender on deep palpation.
- Chest xray – no air under diaphragm.
- AXR – no dilated bowel.

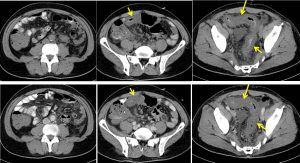
CT scan findings:
- A long segment bowel wall thickening (yellow arrows) is identified involving the rectum extending to mid sigmoid colon. This thickening is regular and no nodularity is seen.
- No obvious enhancement of the bowel wall on post contrast images.
- Presence of mesenteric fat streakiness with tortuous mesenteric vessels are noted.
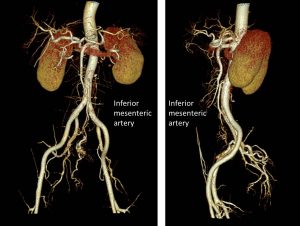
- CTA shows normal inferior mesenteric artery, however its branches are not well seen.
- No extraluminal air to suggest pneumoperitoneum.
- No extraluminal contrast extravasation is identified throughout the abdomen.
- Moderate ascites is seen.
HPE findings:
- Macroscopy: specimen labelled as biopsy of rectosigmoid consist of multiple pieces of yellowish tissue measuring about 4 mm in aggregate.
- Microscopy: levels show multiple fragments of colonic tissue in which focal area show surface erosion of re-epithelialization seen. A few glands towards the surface is atrophic. Goblet cells are depleted. The lamina propria is hyalinized. Fibrin thrombi is also noted. There is no crypt branching or outpouching, cyrptitis, crypt abscess or granuloma present. No pseudomembrane seen. Adjacent neutrophilic exudate is also noted. No dysplasia or malignancy.
- Interpretation: features are suggestive of ischaemic colitis
Discussion:
- Ischaemic colitis refers to inflammation of the colon secondary to vascular insufficiency and ischaemia.
- is the most common vascular disorder of the gastrointestinal tract.
- It typically affects elderly patients, being a frequent cause of rectal bleeding, abdominal pain, and diarrhea.
- Ultrasound is not the standard diagnostic tool for patients with suspected ischaemic colitis. Some related findings include symmetric bowel wall thickening (100%), segmental involvement of the colon (80%), preservation of colon wall stratification (66%), altered pericolic fat (28%), free fluid (19%) and pneumatosis (1.7%).
- CT examination with contrast media is actually considered the main technique for the non-invasive diagnosis of IC and also in cases of acute abdomen of different and various origins, as it is widely available, it can suggest ischaemic colitis when it is unsuspected, can diagnose complications and exclude other illnesses.
- CT findings include bowel wall abnormality (thickening, submucosal odema, bowel dilatation or pneumotosis coli), peritoneal or retroperitoneal abnormality (pericolic fluid or fat stranding, mesenteric oedema, free fluid or pneumoperitoneum) and vascular abnormality (Mesenteric artery or vein occlusion or air in portal vein or mesenteric vein).