
Case contribution: Dr. Radhiana Hassan
Clinical:
- A 57 years old man
- Underlying hypertension and bronchial asthma
- Presented with generalised body itchiness for 2 months
- Associated with jaundice for 2 weeks, tea coloured urine, and loss of appetite
- History of taking traditional medicine
- Clinically no stigmata of liver disease
- Blood investigation shows mixed hepatitis feature that may represent drug induced liver injury
- Hepatitis B and Hepatitis C are negative
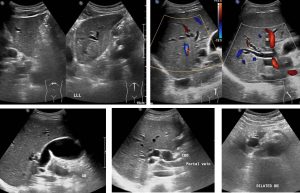
Ultrasound findings:
- Liver is slightly increased in echogenicity. However, the echotexture is normal with smooth margin. The liver measures 12.9 cm in length.
- Gallbladder is well distended with few septations within. A small echogenic lesion is seen within the gallbladder which moves with repositioning. No posterior shadowing. The gallbladder wall is not thickened and no pericholecystic fluid seen.
- The common bile duct, intrahepatic and extrahepatic bile ducts are grossly dilated. The common duct measures about 1.6 cm at porta hepatis. The CBD is traced until head of pancreas, however, no apparent calculus or mass observed. Distal part of CBD is obscured by bowel gas thus limiting the study.
- Portal vein is normal in calibre which measures about 1.1 cm. The visualised pancreas is homogenous and normal in appearance. No obvious mass observed.
- Impression: Dilated biliary system with no apparent obstructive cause is observed.
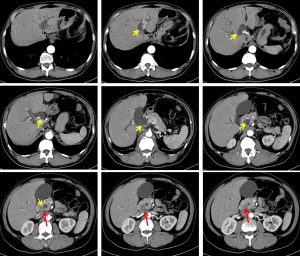
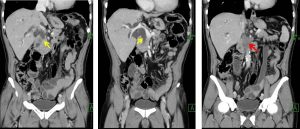
CT scan findings:
- There is gross dilatation of left and right intrahepatic, common hepatic and common bile duct (CBD) yellow arrows. The maximal diameter is at its proximal CBD measures about 1.9 cm. It is seen tapering at its distal part.
- There is an ill-defined enhancing soft tissue mass is noted at pancreatic head measures about 0.5 x 1.7 x 1.8 cm (red arrows). The rest of pancreas is homogenously enhanced with no other focal lesion is seen.
- Pancreatic duct is also dilated. No intraductal lesion or calculus seen.
- Gallbladder, spleen, adrenals and both kidneys are normal.
- Also had liver and bone lesions suggestive of metastasis.
- No significant para-aortic or paracaval nodes enlargement.
- Impression: Pancreatic head mass causing external compression and biliary tree obstruction; highly suspicious of malignancy.
HPE findings:
- Specimen labelled as brush cytology of common bile duct
- Macroscopy: minimal blood stained common bile duct
- Microscopcy: cellular smear. Smear shows malignant cells arranged in sheets, clusters, singly dispersed and some forming glandular architecture. The malignant cells display moderate pleomorphism, hyperchromatic nuclei with some shows prominent nucleoli. Occasional mitosis are seen. In areas, sheets of benign ductal cells are also present.
- Interpretation: adenocarcinoma.
Progress of patient:
- ERCP done shows bulging ampulla with grossly dilated extra and intrahepatic duct, stenotic distal CBD about 6 cm in length. A self-expanding metallic stent inserted and well expanded.
- EUS shows multiple lymph nodes at coeliac axis and periportal area. Tumour infiltrating into CBD and embarking portal vein.
- Impression: non-resectable pancreatic tumour
- Palliative chemotherapy given
Diagnosis: Pancreatic cancer (adenocarcinoma)
Discussion:
- Pancreatic cancer is a common gastrointestinal malignancy.
- It is slightly more common in men, and is usually a disease of older adults.
- Cigarette smoking appears to be one of the strongest risk factors, and is likely associated with as many as one quarter of all pancreatic tumors.
- Other known risk factors include diabetes mellitus, alcohol use, obesity, and various genetic syndromes.
- More than 95% of malignant neoplasms of the pancreas arise from the exocrine portions of the gland (ductal and acinar cells), and demonstrate features consistent with adenocarcinoma.
- Location of cancer is mainly at head and uncinate process; 2/3 of cases.
- Ultrasound show non-specific findings.
- CT of typical ductal adenocarcinomas appear as poorly defined masses which enhance poorly compared to adjacent normal pancreatic tissue and thus appear hypodense on arterial phase scans in 75-90% of cases, but may become isodense on delayed scans (thus the need for multiple phase scanning when pancreatic cancer is the clinical question).
-
CT correlates well with surgical findings in predicting unresectability (positive predictive value of 89-100% ). The most important feature to assess locally is the relationship of the tumor to surrounding vessels (SMA and celiac axis). If the tumor surrounds a vessel by more than 180 degrees, then it is deemed unresectable.

Recent Comments