
Case contribution: Dr Radhiana Hassan
Clinical:
- A 71 years old man
- Underlying DM, HPT, IHD and gastritis on medication and regular follow up
- Presented with abdominal pain for 2 days
- Localized at right hypochondriac region, non-radiating.
- Feeling feverish but no documented increased temperature
- Also had vomiting. No jaundice, no loss of appetite or loss of weight
- Per abdomen soft, tender over right hypochondriac region, liver palpable, murphy sign positive
- TWBC=17, Hb 13 and Plt 370
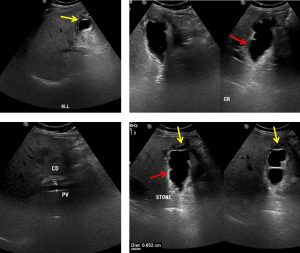
Ultrasound findings:
- There is no focal lesion in the liver. No intra- or extrahepatic duct dilatation.
- Gallbladder is adequately dilated. Multiple small calculi are seen within the gallbladder neck. No sludge seen within the lumen.
- The gallbladder wall is thickened measuring 0.6 cm in diameter (red arrows). Minimal pericholecystic fluid is detected (yellow arrows).
- Echogenic foci with comet tail artifacts are seen at the fundus of the gallbladder.
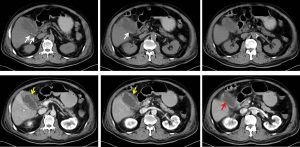
CT scan findings:
- The gallbladder is distended with homogenous fluid (HU 2-5).
- Multiple hyperdense calculi and internal septation are also seen within.
- It has irregular thickened and enhancing wall.
- There is a focal defect at the superior aspect body of the gallbladder (red arrows). Communication with the surrounding pericholecystic fluid is seen suggestive of perforation. Associated adjacent fat streakiness is also seen.
- No mass is seen within the gallbladder. Common bile duct is not dilated.
- Other organs are normal.
Operative findings:
- Adhesion between transverse colon, duodenum with gallbladder, distended gallbladder
- Multiple necrotic areas at body and fundus of gallbladder, noted pus at gallbladder bed
- Short cystic duct
- Duodenum serosal tear, necrotic patch at duodenum, repair done
- Cholecystectomy done. Gallbladder opened, shows thickened wall and small pigmented stones within. Dirty bile and pus. No mass seen
HPE findings:
- Macroscopy: specimen labelled as cholecystectomy consist of surgically cut open congested gallbladder measuring 90x42x30 mm. There are multiple blackish stones within the lumen. The wall thickness is 6-14 mm. No tumour cells seen. The external surface of the gallbladder shows dusky appearance. There are multiple necrotic patch over body and fundus area. There is also perforation site over the fundus area. The inner surface of the gallbladder is velvety in appearance. Multiple blackish stones in the lumen of the gallbladder measuring 2-5mm in diameter.
- Microscopy: sections of the gallbladder show extensive mucosal ulceration. In areas there is transmural necrosis of the gallbladder wall. The underlying stroma show a dense mixed acute and chronic inflammatory cell infiltrate. These are Rokitansky Aschoff sinuses seen withih the muscular layer. The blood vessels are congested. No evidence of dysplasia or malignancy seen.
- Interpretation: cholecystectomy consistent with empyema.
Diagnosis: Perforated gallbladder empyema
Discussion:
- Empyema of the gallbladder is a complication of cholecystitis
- It refers to situation where gallbladder lumen is filled and distended by pus
- It is also known as suppurative cholecystitis
- Ultrasound findings are not specific. It may show sonographic features of cholecystitis with or without calculus within the lumen.
- CT scan shows feature of cholecystitis with high-attenuation material within the gallbladder lumen that represent pus. But the finding is nonspecific and often difficult to differentiate from sludge
Recent Comments