
Case contribution: Dr Radhiana Hassan
Clinical:
- A 49 years old lady
- History of left neck swelling for 10 years, rapid progressive in size for the last 3 years
- No hoarseness of voice, no snoring, no LOA, no LOW and no thyroid symptoms
- Clinically a left thyroid swelling 10×10 cm, firm, non-tender, mobile, able to get below it, no retrosternal extension, no carotid bruit
- Thyroid function test normal, vocal cord assessment is also normal

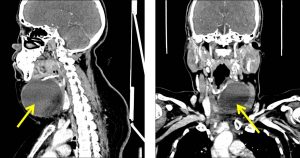
Radiographic findings:
- There is a largesoft tissue density at anterior neck, more towards the left side (yellow arrows).
- No calcification seen within. No fluid levels.
- It causes trachea displacement towards the right.
- No significant anterior trachea compression is seen on lateral view.
- No apparent extension into the retrosternal area inferiorly.
- No associated bony erosion or bone destruction.
- The visualized lung apices are clear.
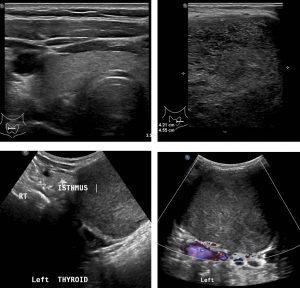
Ultrasound findings:
- Right thyroid is normal in size, homogeneous and shows smooth echotexture.
- No focal mass or cyst is seen in the right thyroid gland.
- Isthmus is mildly enlarged measuring 0.5 cm in width.
- A large well defined hypoechoic lesion is seen within the left thyroid gland.
- There are multiple echogenic foci within it and fill the entire nodule.
- On Doppler, no colour flow seen within the nodule.
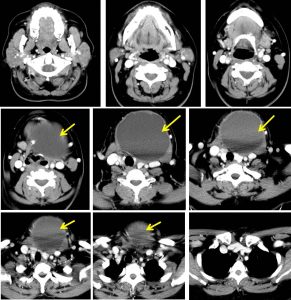
CT scan findings:
- There is a well-defined large left paramedian rounded hypodense cystic mass (HU range 10-32) at anterior neck, measures about 8.4 x 8.8 x 7.3 cm.
- No intralesional calcification or internal septation.
- It is seen just inferior to the hyoid bone and extending inferiorly to the supramediastinum level
- No retrosternal extension.
- The mass closely abuts the left thyroid lobe, and causing right lateral displacement of the thyroid gland. However, clear margin is still seen in between, with no actual claw sign is seen.
- The rest of thyroid glands are homogenous.
- Right strap muscle appears elevated, with non-visualized of the normal left strap muscle appearance; possible suggest origin of the mass.
- Bilateral distal sternocleidomastoid muscles are splayed laterally by the mass.
- There is trachea deviation to the right with no significant narrowing is observed.
- The left internal jugular vein (IJV) and left common carotid artery (CCA) are patent.
- No significant enlargement of the cervical lymph nodes.
Intra-operative findings:
- Large cystic mass 10×10 cm at anterior neck overlying the thyroid gland
- Densely adhered to strap muscle
- Involving the hyoid bone, no plane seen
- Cyst ruptured during manipulation, brownish cystic content noted
HPE findings:
- Macroscopy: specimen labelled as thyroglossal cyst with part of hyoid bone consist of a collapsed greyish cyst measuring 75x90x40 mm with of bony tissue. Cut section shows a uniloculated cyst with wall measures 4-10 mm in thickness. No solid areas seen. The bony tissues are unremarkable.
- Microscopy: sections show fibro-collagenous cyst wall predominantly devoid of epithelial lining, replaced by mixed inflammatory cells infiltrate and focally lined by non-keratinizing squamous epithelium. The stroma are mild to moderately infiltrate by mixed inflammatory cells consisting of lymphocytes, foamy macrophages, plasma cells and scattered neutrophils. In areas, groups of benign thyroid follicles are noted. The bony tissue are unremarkable. Negative for malignancy.
- Interpretation: consistent with thyroglossal duct cyst.
Diagnosis: Thyroglossal duct cyst.
Discussion:
- Thyroglossal duct cysts are the most common congenital neck cysts
- The cysts are typically located in the midline and the most common midline neck mass in young patient.
- Majority presents during childhood (90% before 10 years of age)
- Associated with ectopic thyroid in 40% of cases.
- The cysts can occur anywhere along the course of thyroglossal from foramen of cecum to the thyroid gland.
- The cyst is typically located in the midline (about 70%) of cases, those off-midline characteristically adjacent to the thyroid cartilage and almost all are located within 2 cm of the midline.
- On ultrasound, the features depends on whether infected or non-complicated cyst. A soft tissue lesion in association with the cyst may be ectopic thyroid tissue or rarely represent carcinoma
- On CT scan it is usually thin-walled, well-defined homogenous fluid density lesion with an anterior midline or paramedian location. It may demonstrate slight capsular enhancement.The sternocleidomastoid muscles are typically displaced posteriorly or posterolaterally.
- Differential diagnosis:
- Branchial cleft cyst- less common and usually well away midline
- Epidermoid cyst- superficial to strap muscles, usually tethered to underlying tissue and not mobile
- Thyroid cyst or neoplasm
- Parathyroid adenoma
- Ranula- a rare benign acquired cystic lesion at floor of mouth
- Laryngocele-usually acquired than congenital due to increased intralaryngeal pressure, seen as well-dfeined air or fluid containing lesion at upper cervical paralyngeal soft tissue
- Lymphadenopathy
- Lipoma
Recent Comments