
Case contribution: Dr Radhiana Hassan
Clinical:
- A 31 years old lady
- No known medical illness
- Presented with a rapidly growing mass at volar aspect of left forearm.
- Clinically, a mass felt at left forearm, 7×8 cm, firm with no distal neurovascular deficit.
- No other positive findings
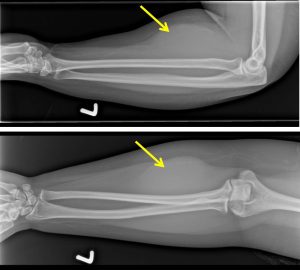
X-ray findings:
- There is lobulated soft tissue opacity seen at the volar aspect of the left forearm, medial to left ulnar bone (yellow arrows).
- No calcification is seen within. No fluid levels.
- No lytic or sclerotic bone lesion.
- No joint erosion or joint dislocation.
- Overlying skin is unremarkable.
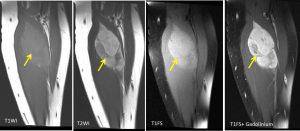

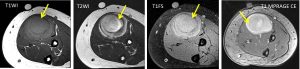
MRI findings:
- A large well-defined lobulated intra-muscular soft tissue mass is seen at anterior compartment of the proximal left forearm.
- The mass is located within the superficial volar compartment, most likely within the pronator teres muscle.
- The mass returns slightly hyperintense signal intensity compared to muscle on T1 and heterogenous mixed signal (mostly hyperintense) on T2.
- No appreciable fat component observed with no appreciable signal suppression seen on the fat saturated sequences.
- Heterogeneous enhancement observed post IV Gadolinium.
- No blooming artefact seen on GRE sequences to suggest the presence of either calcification or haemosiderin deposits (images not shown).
- This mass is causing expansion of the muscle bulk causing mass effect to the surrounding structures with displacement of flexor carpi radialis muscle medially. It is seen abutting the radial neurovascular bundle medially, however, no compression or nerve entrapment seen. No obvious abnormal signal intensity is seen within the radial neurovascular bundle.
- Clear plane of demarcation with surrounding muscles and subcutaneous tissue. No thickening of overlying skin.
- No extension to the muscles or bone.
HPE findings:
- Macroscopy: specimen labelled as soft tissue left forearm consist of a multiple pieces of whitish tissue measuring 20 mm in aggregate diameter.
- Microscopy: section shows multiple fragments of lesional tissue admixed with skeletal muscle fragments and fibrocollagenous tissue. The lesional tissue is hypercellular and composed of proliferation of uniform spindle-shaped cells arranged in fascicles. The cells display bland elongated and slender nuclei, inconspicuous nucleoli, and eosinophilic cytoplasm. No mitosis or atypical cells are seen. The stroma is collagenized. Some of the blood vessels are ectatic with foci of hemorrhage.
- Immunohistochemistry: the cells are diffusely positive for SMA with focal nuclear positivity for b-catenin. The cells are negative for desmin, s100 and cd34.
- Interpretation: soft tissue spindle cell neoplasm with fibroblastin/myofibroblastic differentiation. The morphological and immunohistochemical features are consistent with fibromatosis.
Diagnosis: fibromatosis
Discussion:
- Fibromatosis refers to a wide range of soft tissue lesions that can share histopathologic pattern of fibrous tissue proliferation.
- It can occur at any anatomic sites and vary in their behaviour from benign to malignant.
- Musculoskeletal fibromatoses can be divided into superficial and deep groups.
- The superficial fibromatoses are typically small, slow-growing lesions and include palmar fibromatosis, plantar fibromatosis, juvenile aponeurotic fibroma, and infantile digital fibroma.
- The deep fibromatoses are commonly large, may grow rapidly, and are more aggressive. They include infantile myofibromatosis, fibromatosis colli, extraabdominal desmoid tumor, and aggressive infantile fibromatosis.
- Radiographs typically reveal a nonspecific soft-tissue mass, and calcification is common only in juvenile aponeurotic fibroma.
- MR imaging may show characteristic features of prominent low to intermediate signal intensity and bands of low signal intensity representing highly collagenized tissue. However, fibromatoses with less collagen and more cellularity may have nonspecific high signal intensity on T2-weighted images.
- Involvement of adjacent structures is common, reflecting the infiltrative growth pattern often seen in these lesions
Recent Comments