
Case contribution: Dr Radhiana Hassan
Clinical:
- A 21 years old man with no past medical illness
- Presented with hearing loss for one year
- Associated with right ear discharge and tinnitus. Also had occasional headache.
- No high risk behaviour
- No fever, no cough, no vomiting, no fitting episode
- Referred for further management from another hospital with initial diagnosis of cholesteatoma
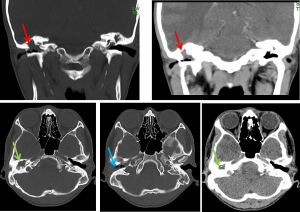
CT scan findings:
- There is complete opacification of the right middle ear and right mastoid (red arrows) by with minimally enhancing soft tissue lesion.
- The external ear is also partially filled by the same lesion (blue arrow).
- The mastoid septa as well as middle ear structure including the ossicles are eroded (green arrows) causing the mastoid and middle ear to be one common cavity.
- Tegmen tympani, tegmen mastoidum and sigmoid plate are intact.
- The scutum is minimally eroded and normal tympanic membrane is not seen.
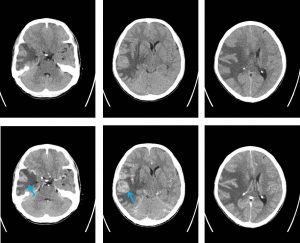
- Brain shows white matter oedema with enhancing lesion within the right temporal lobe
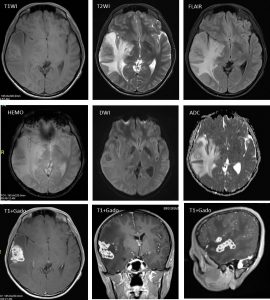
MRI findings:
- Multiloculated intraparenchymal lesions are seen at the right frontal and temporal region. The periphery of the lesion generally appears hyperintense to cortex on T1, isointense on T2 and FLAIR; while centrally these appear hypointense on T1, T2 and FLAIR.
- Most of the lesions show peripheral rim enhancement, while some part of the lesions especially the ones involving dura show homogenous enhancement post IV Gadolinium.
- No area of restricted diffusion is observed on DWI/ADC.
- The adjacent dura appears thickened and enhancing.
- Marked perilesional vasogenic oedema is visualized which involves the right temporal, frontal and parietal lobes with effacement of the cerebral sulci.
- The right lateral and 3rd ventricle is compressed with midline shift of about 1.0 cm to the left and subfalcine herniation.
- Both temporal horns of lateral ventricles and occipital horn of the left lateral ventricle appears prominent. 4th ventricle is not dilated. No tonsillar herniation detected.
Progress of patient:
- EUA of right ear with modified radical mastoidectomy and left myringotomy and T-tube insertion, direct larygoscopy and biopsy
- Right middle ear tissue positive AFB smear
- Epiglottis positive AFB smear
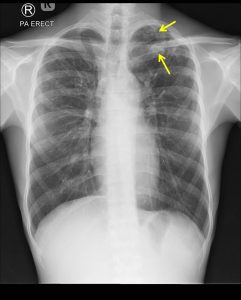
- Sputum AFB negative, Chest radiography shows cavities at left upper lobe
- Started on anti TB
Diagnosis: Disseminated Tuberculosis
Discussion (Tuberculous otomastoiditis):
- Tuberculous otomastoiditis is an uncommon form of acute otomastoiditis secondary to tuberculosis infection
- It can present with wide range of presentations including painless chronic otorrhoea, purulent discharge, ossicular erosion and cervical nodes enlargement
- The early diagnosis is not easy because of its low prevalence and ambigous clinical signs.
- Delay in diagnosis causes permanent hearing loss and facial nerve paralysis.
- Amongst the common reported HRCT findings include soft tissue lesion in entire middle ear cavity, preservation of mastoid air cells without sclerotic change, soft tissue extension to external ear canal with mucosal thickening and relative non-erosion of scutum compared to usual findings of cholesteatoma.
Recent Comments