
Clinical:
- A 28 years old lady
- First 2 presentations were optic neuritis
- Third presentation with lower limbs weakness
- Current presentation with bilateral lower limb weakness and urgency.
- Clinical examination shows bilateral lower limb power 4/5.
- Sensory level reduction at T2-T11 and L5-S1.
MRI findings:
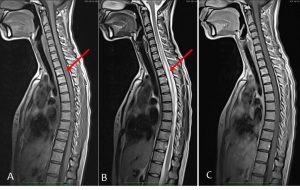
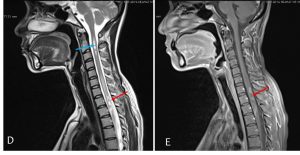
- Initial MRI shows diffuse long segment high signal intensity within the cord (yellow arrows) with superior most margin at C4/C5 level and inferior margin at T8/T9 level. Faint abnormality also seen at C2-C3 level. There is no enhancing lesion on post Gado.
- Repeat MRI during current admission shows lesion at C2-C3 level, more conspicuous and almost of CSF density as compared to previous MRI. It is already hypointense on T1. No cord expansion.
- Hyperintense signal is also seen at C5 to T8 level, similar extension of involvement as compared to previous findings.
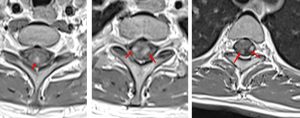
- However, there are multiple foci of enhancement seen at level of C7 to T2 on post contrast (red arrows). These enhancing lesion are peripherally and mostly posterolateral in location.
- There is cord expansion with the largest AP diameter of the spinal cord measures 0.7cm at T2 level
- MRI brain is normal (images not shown).
Diagnosis: Correlating with clinical presentations, features are in consistent with neuromyelitis optica.
Discussion: Neuromyelitis optica (NMO)
- NMO is an idiopathic, autoimmune, inflammatory, demyelinating condition
- It is characterised by bilateral optic neuritis and myelitis resulting in blindness and paraplegia
- Involvement of optic nerve and spinal cord is common
- The brain and brainstem are generally spared (10%)
- 23% mortality rate
- Women in their 30s and 40s
Comparison Neuromyelitis optica and multiple sclerosis:
| NMO | MS |
| More severe presentations with poor recovery (irreversible impairment) | Mild to moderate presentations |
| Optic nerve and spinal cord | Multiple lesions in the brain |
| Free of oligoclonal bands | Oligoclonal bands |
| NMO-IgG (73% sensitivity) | Seronegative on NMO-IgG |
| Attack water channel in astrocytes | Attack immune T-cell |
| CSF: more cell response | CSF: normal cell count, even during exacerbations |
| Women:men=4:1 | Women:men=2:1 |
| Late 30s | Early 20s |
| Non-caucasian background | Northern europe/caucasian |
Recent Comments