
Clinical:
- A 47 years old lady
- Came for screening mammogram
- Asymptomatic
- No family history of cancer
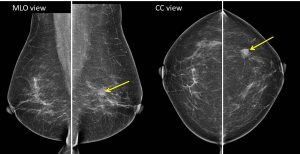
Bilateral mammogram in MLO and CC views Mammogram findings:
- Bilateral fatty breasts (Birads a) with symmetrical parenchymal pattern.
- There is a speculated mass seen at left upper outer quadrant.
- This lesion measured about 10 mm in largest diameter.
- Associated stromal distortion seen.
- No suspicious clustered microcalcification. No skin changes or nipple retraction. No abnormal axillary nodes.
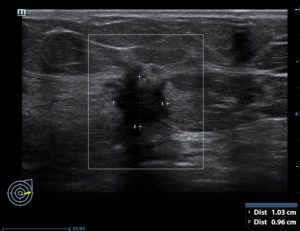
Ultrasound findings:
- There is a hypoechoic lesion at Lt2-3H measuring about 10×10 mm in size.
- It showed speculated margin with ‘finger-like’ projection.
- Posterior shadowing and presence of penetrating vessels are also seen.
- No other lesion is seen in both breasts. No dilated duct.
- No abnormal axillary node.
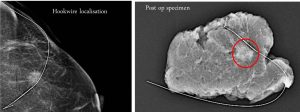
US-guided hookwire localisation done prior to wide local excision:
- Mass lesion is identified using ultrasound noted to be at about 3H location.
- Procedure performed under aseptic technique.
- Puncture using Kopan hookwire needle done under ultrasound guidance.
- J-tip secured about 2.0 cm from the mass lesion.
- Mammogram done post hookwire localisation showed the tip is about 2 cm from the edge of the lesion.
- No complication noted immediately after the procedure.
- Post procedural specimen shows mass lesion removed with surrounding tissue.
HPE result:
- Invasive carcinoma of no special type, Grade 2
- TNM stage T1N1aMx
- Tumour cells are seen at medial margin, other margins (superficial, deep, superior, inferior and lateral margins are free
- Left axillary clearance: 1 out of 13 lymph nodes with evidence of metastasis.
Progress of patient:
- Referred to other hospital for further treatment.
- Planned for re-excision for non-clear margin
Discussion (Hookwire localisation):
-
Pre-operative hookwire localization is part of surgical management of non-palpable breast lesions
-
It can be done using mammography, ultrasound or MRI guidance.
-
There is no specific preparation for this procedure, however since operation usually planned few hours after the procedure, patient is prepared for the operation.
-
Recent mammograms, ultrasounds or MRI scans and the reports, should be available to be reviewed by the radiologist before the procedure.
-
Procedure is performed under aseptic technique with local analgesia.
-
Once the needle is in the correct position, a fine wire is passed down the centre of the needle and the needle is removed, leaving the wire in place.
-
A final mammogram/ultrasound is carried out to show the surgeon where the tip of the wire lies in relation to the abnormality that is to be removed (a mammogram provides a better visual image for the surgeon of where the tip of the wire lies than ultrasound).
-
Some surgeons prefer marking on the skin of the patient of where the tip of wire.
-
After the procedure, part of the wire that is sticking out from breast tissue is taped down to the skin, and the hookwire remains in the abnormality in the breast.
-
Patient is pushed to OT with previous imaging and the images from the breast hookwire localisation will be sent together to the operating theatre, so that the surgeon can refer to them.
-
The surgeon will remove the wire together with the abnormality at the time of the operation.
-
Specimen is sent back to radiology department to confirm removal of lesion.
Recent Comments