
Clinical:
- A 50 years old man
- Long standing poorly controlled hypertension
- Presented with shortness of breath
- No fever and no cough
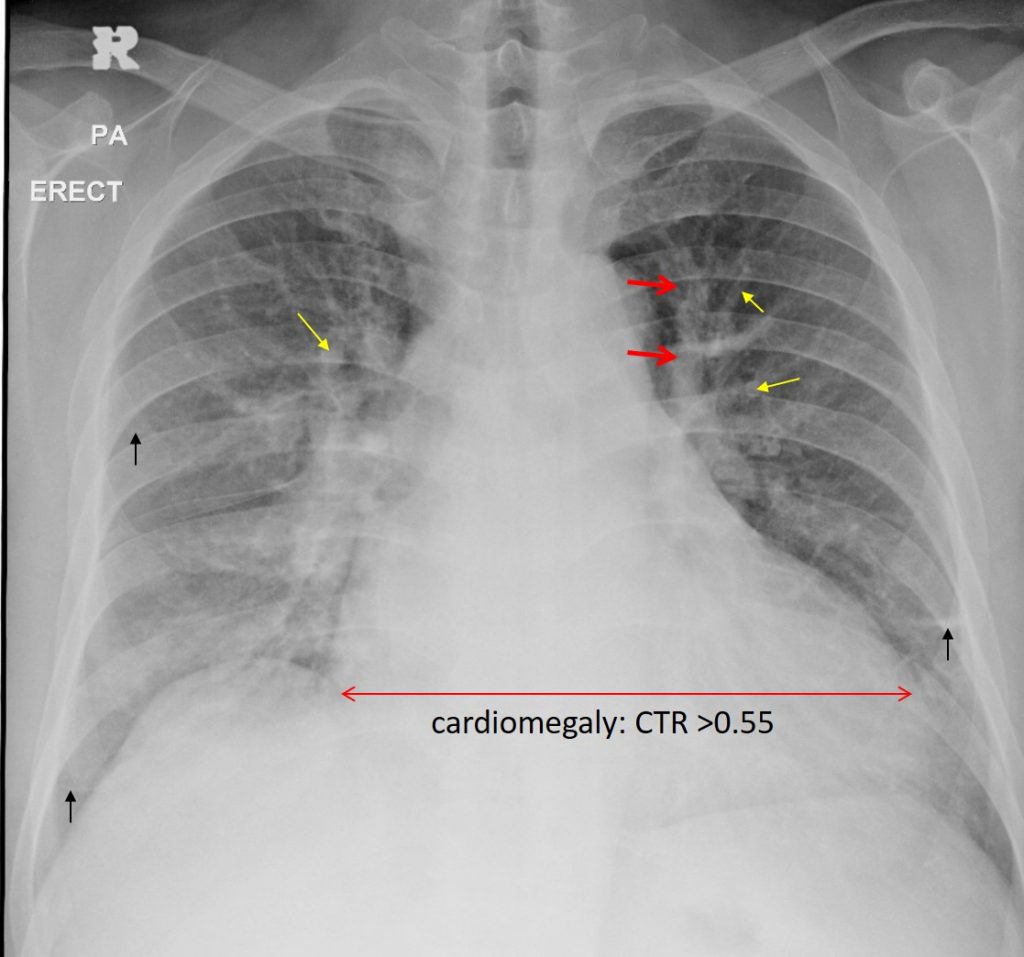
Radiographic findings:
- There is cardiomegaly evidenced by increased cardiothoracic ratio
- Presence of upper lobe diversion, more prominent on the left side (red arrow)
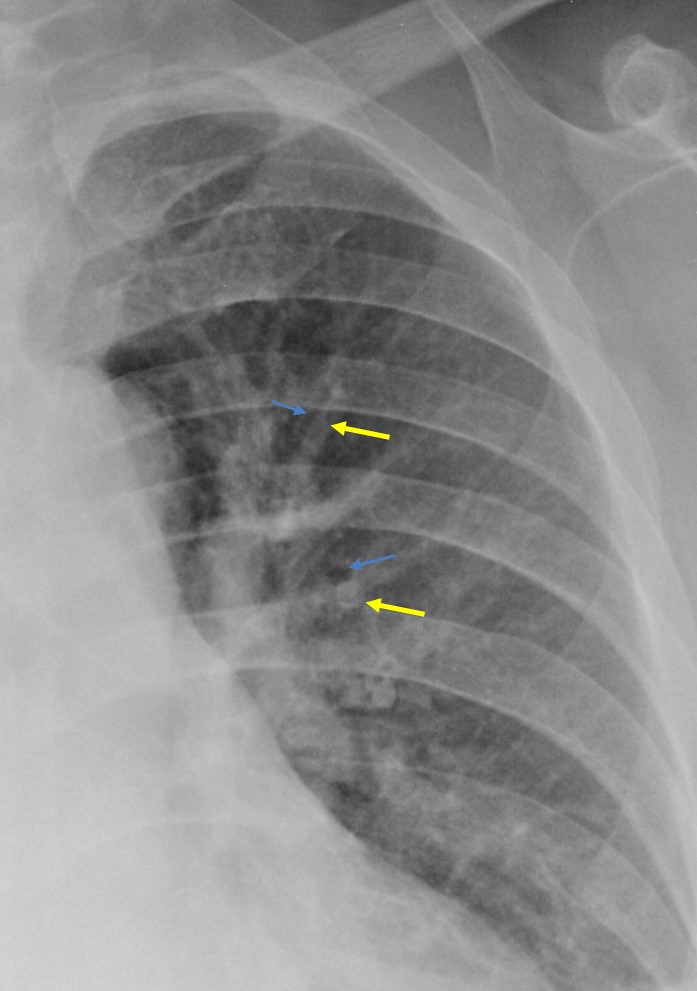
- Increased artery (yellow arrows) to bronchus (blue arrows) ratio are also seen at both upper and mid zones
- Presence of peripheral septal thickenings (Kerley B) lines (black arrows)
- Minimal consolidation at right perihilar region
- No pleural effusion
Diagnosis: Congestive cardiac failure.
Discussion (Upper lobe diversion):
- Upper lobe diversion is a sign seen on upright chest radiograph.
- It is also known as upper zone redistribution or cephalisation
- In these patients, minimal early perivascular oedema develops first in the lower zone, leading to contraction of the lower zone arteries and veins and a relative increase in the upper zones.
- The comparison vessels should be equidistant from the hilar point done on upright chest radiograph.
- This sign produces dilated branching and branching upper zone pulmonary veins resembling the antlers of a stag, thus another name for this sign is stag-antler’s sign
Recent Comments