
Case contribution: Dr Radhiana Hassan
Clinical:
- A 36 years old lady
- Born with congenital craniofacial anomaly.
- Left eye is blind.
- History of fenestration of septum pellucidum of dilated ventricle.
- Current admission for recent onset of headache and two episodes of breakthrough seizures
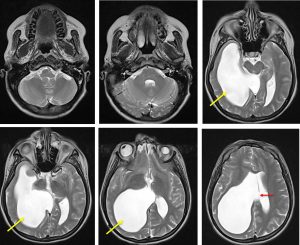
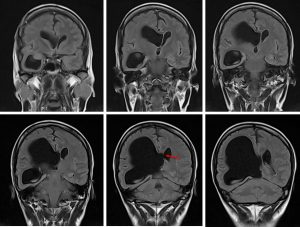
MRI findings:
- Right lateral ventricle is grossly dilated (yellow arrows) with ballooning of the occipital and temporal horns.
- Resultant mass effect with midline shift to the left of about 8 mm.
- Evidence of disruption of the septum pellucidum in keeping with previous fenestration procedure (red arrows).
- Inferiorly is causes slight compression to the right midbrain.
- There is compression with thinning of the brain parenchyma on the ipsilateral side
- No periventricular hyperintensity to suggest CSF seepage of acute hydrocephalus.
- Small left globe with smaller left optic nerve.
Diagnosis: Unilateral ventriculomegaly, post fenestration done.
Discussion:
- Unilateral hydrocephalus is asymmetrical dilatation of one lateral ventricle caused by obstruction of foramen of monro, and is distinct from unilateral ventricular enlargement caused by asymmetrical cerebral hypoplasia or atrophy.
- Various modes of treatment have been advocated for this condition. These include placement of shunt CSF diversion from dilated ventricle, fenestration of septum pellucidum by open craniotomy and fenestration of septum pellucidum by stereotactic method
- Fenestration of septum pellucidum:
- To establish flow
- Avascular area above and anterior to the fornix will be chosen
- In cases with cavum septum pellucidum both leaflet should be opened and coagulated
- Contralateral frontal horn should be identified before termination of procedure
Recent Comments