
Case contribution: Dr Radhiana Hassan
Clinical:
- A 30 years old lady
- No knowm medical illness
- Presented with epigastric pain for one month
- Became severe with nausea and non-billous vomiting
- She was pregnant at 30 weeks, Gravida 2
- Clinically patient was tachypnoeic and in severe pain
- Other vital signs were stable
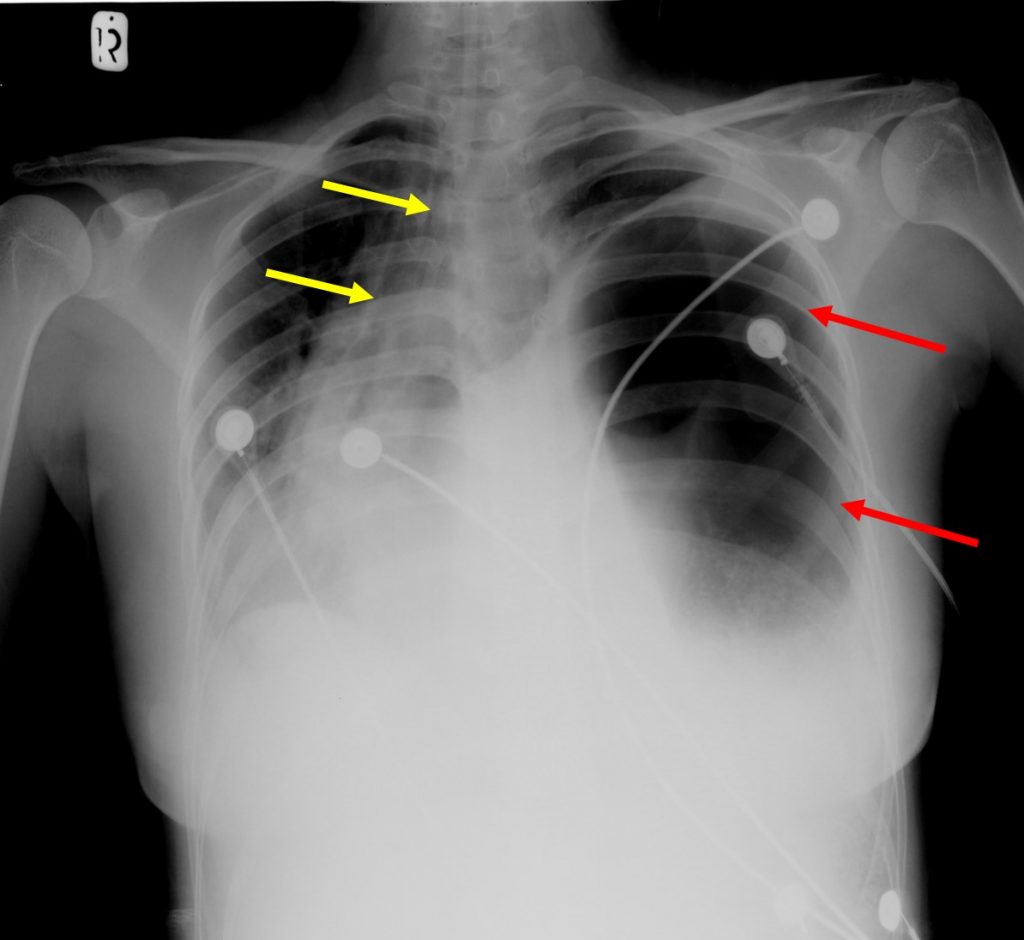
Chest radiograph findings:
- A large lucent lesion seen occupying the left hemithorax (red arrows)
- It shows thick wall with no fluid levels within
- Left hemidiaphragm is not well visualized
- The trachea and mediastinum is shifted to the right side (yellow arrows)

CT scan findings:
- Herniation of stomach (yellow arrows), bowel loops and mesentery (red arrows) are seen into left hemithorax
- It occupies almost the whole left thoracic cavity
- Mediastinal shift to the right side
Intra-operative findings:
- An emergency laparotomy was performed
- A gush of air during the initial opening of peritoneum with peritoneum contaminated with bowel content.
- The distal part of the stomach, the whole large bowel, small bowel and appendix were found inside the hemithorax
- A 6×4 cm defect at posterolateral aspect of hemidiaphragm
- The greater curvature of stomach was ischaemic and a 2×3 cm perforation seen
Diagnosis: Adult diaphragmatic hernia
Discussion:
- Diaphragmatic hernias are defined as either congenital or acquired defect in the diaphragm
- Congenital diaphragmatic hernia divided into 1) Bochdalek hernia-The most common type of diaphragmatic hernia (95%), located posterolaterally and usually present in infancy and 2) Morgagni hernia- anterior, smaller and present later in life
- Acquired hernias are 1) Traumatic diaphragmatic hernia 2) Hiatus hernia and 3) iatrogenic hernia
- Based on the location of the defect seen in this case, this is most probably undiagnosed Bochdalek hernia
Recent Comments