
Case contribution: Dr. Radhiana Hassan
Clinical:
- An 87 years old lady
- Underlying DM and HPT.
- Presented with left sided body weakness.
- Associated with slurred speech.
- On examination E3V2M6. Power left upper and lower limb 0/5.
- BP 239/112 mmHg.
CT scan findings:
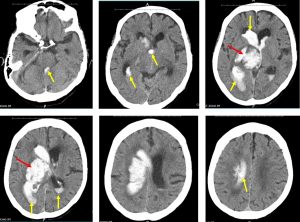
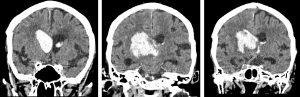
- There is a large hyperdensity in the right basal ganglia (red arrows) measuring about 4.3x 4.4×4.3 cm (AP x W x CC) in keeping with acute hemorrhage.
- There is extension of hemorrhage into the lateral, third and fourth ventricles (yellow arrows).
- Midline shift to the left measuring about 10 mm.
- Effacement of the adjacent cerebral sulci.
- Underlying cerebral atrophy.
Diagnosis: Acute right basal ganglia hemorrhage with intraventricular extension.
Discussion:
- Basal ganglia hemorrhage is a common form of intracerebral hemorrhage
- It is a neurologic emergency that requires immediate imaging and neurosurgical referral
- The most common cause is poorly controlled long-standing hypertension
- Typically seen on CT scan as a region of hyperdensity centered on the basal ganglia or thalamus. Not infrequently there may be an extension into the ventricles.
- Volume of the hemorrhage may be estimated by APxWxCC/2 formula, which may have neurosurgical and prognostic implications (only parenchymal hemorrhage not intraventricular extension).
- The mainstay of treatment is medical, with control of hypertension and attempts to prevent secondary cerebral injury.
- If an intraventricular hemorrhage is present then hydrocephalus is a common sequelae and CSF drainage with an extra-ventricular drain is often needed.
- Evacuation of the clot is controversial and only potentially useful in large (>60 mL) hemorrhage.
Recent Comments