
Case contribution: Dr Radhiana Hassan
Clinical:
- A 62 years old lady
- Underlying DM and HPT on medication, morbid obesity BMI 38, body weight 80 kg
- Presented with left flank pain for one day, radiating to the back, pain score 5/10
- Associated with vomiting and feeling feverish
- Similar pain on and off for about one month
- Clinically not septic looking, vital signs stable (BP=144/76), HR 72 bpm, DXT=11
- Abdomen soft, mild tenderness at epigastric and left hypochondriac, renal punch negative
- Given tramadol stat dose, metoclopramide, ranitidine and MMT in ED
- One day after admission, BP drop 81-92, 54-56, not picking up on fluid resuscitation
- HR 102 bpm
- Admitted to ICU, started on noradrenaline
- Intubated, CVP line inserted


Ultrasound findings:
- Bilateral kidneys are normal in shape, size and echogenicity.
- The BPL of right kidney is 10.7 cm and left kidney is 10.8 cm.
- Mild to moderate left hydronephrosis and left proximal hydroureter is noted.
- Unable to trace the distal ureter due to bowel gaseous shadow.
- No focal lesion or perinephric collection bilaterally.
- Urinary bladder is normal.
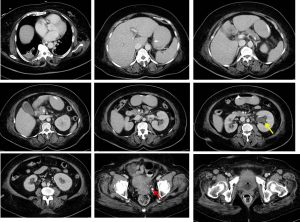
CT scan findings:
- No intra-abdominal collection.
- Left kidney is bigger compared to right kidney.
- Minimal fat stranding at left perinephric region.
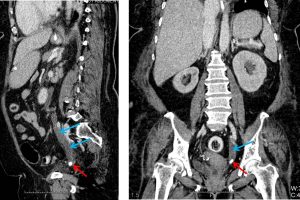
- Moderate left hydronephrosis and hydroureter (yellow arrows). The density of hydronephrosis measures HU:5-11. No fluid levels, air pockets seen within the collecting system. No abnormal enhancement of ureteric wall/lining.
- A calculus is seen in the distal ureter (red arrows) measuring about 1.3×0.7 cm.
- Urinary bladder is not well distended. No obvious focal lesion within.
- Bowel loops are grossly normal. Uterus is normal. No adnexal mass.
- No abnormal lymphadenopathies.
- Right consolidation and left atelectasis of lung bases.
Progress of patient:
- Urgent bilateral retrograde pyelopgram and stenting done in OT
- Left gross hyodroureter and hydronephrosis, pus aspirated
- Stented
- Culture of blood, urine and pus: E. coli
- Urine C& S: candida species
- Discharged well after 16 days admitted
Diagnosis: Urosepsis/septic shock due to pyonephrosis
Discussion:
- This case illustrate the limitation of CT evaluation to distinguish simple hydronephrosis from pyonephrosis
- Fluid attenuation measurements are not reliable.
- And as in this case, no other CT features are present to suggest pyonephrosis.
- In clinical setting, pyonephrosis should be suspected when the clinical symptoms of fever and flank pain are present, combined with radiologic evidence of urinary tract obstruction.
- Emergent diagnosis and prompt treatment is very important for good outcome
- Complications of pyonephrosis include sepsis, xanthogranulomatous pyelonephritis, renal abscess, perinephric abscess and fistula.
Recent Comments