
Case contribution: Dr Radhiana Hassan
Clinical:
- A 34 years old lady
- Incidental findings of abdominal mass during subfertility check up
- Otherwise patient is asymptomatic
- Clinically no mass palpable
- Ultrasound shows a huge cystic mass in the abdomen
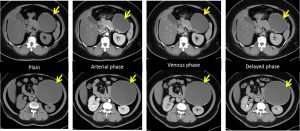
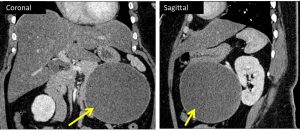
CT scan findings:
- A huge solitary, well circumscribed round lesion is seen arising from the tail of pancreas (yellow arrows)
- It measures about 12.4 x 13.1 x 12.1 cm (AP x W x CC).
- It is unilocular thin-walled predominantly cystic lesion and demonstrates wall enhancement post contrast.
- Clear plane of demarcation is observed with adjacent structures.
- No fat component, calcification or solid component within.
- No surrounding fat stranding or free air pocket is detected.
- No fluid-fluid level. No communication with pancreatic duct is observed, which does not appear dilated.
- No abnormal lymph nodes enlargement
Progress of patient:
- Exploratory laparotomy done
- Intraoperative findings: left sided retroperitoneal cystic tumour, 14x15cm, moderate adhesion between surface of tumour and surrounding soft tissue, tip of pancreatic tail is adhered to the posterior wall of the tumour, splenic hilum is away from the tumour, no abnormal lymph nodes seen
- Excision of retroperitoneal tumour and cholecystectomy done
HPE findings:
- Macroscopy: specimen labelled as retroperitoneal cystic lesion, consist of a well encapsulated cystic mass measuring 120x120x140 mm. Cut section shows uniloculated cyst filled with brownish fluid. Cyst wall thickness measuring 2-4 mm. There is no solid component seen.
- Microscopy: sections show a well encapsulated cystic lesion with extensive area of hemorrhage and necrosis. In focal areas, viable tumour cells are present at the periphery composed of monomorphic cells arranged radially around fibrovascular stalks resembling rosette. The nuclei contain fine chromatin and small nucleolus. The stroma is myxoid in areas. No mitosis is observed. In other areas, remnant of pancreatic tissue is identified.
- Immunohistochemical staining: CKAE1/AE3 and chromogranin are negative, Vimentin and Synaptophysin are positive
- Impression: Suggestive of solid pseudopapillary neoplasm of pancreas
Diagnosis: Solid pseudopapillary tumour of pancreas
Discussion:
- It is a rare pancreatic tumour; comprises 1-2% of exocrine pancreatic tumours
- It tends to occur in young females 2nd-3rd decade of life
- It is usually benign, but malignant degeneration does occur
- Most patients are asymptomatic at presentation
- Lesions can be large at the time of diagnosis (median size 8 cm)
- There is predilection to occur at pancreatic tail
- SPT of the pancreas with clear criteria of malignancy: vascular and nerve sheath invasion or lymph node and liver metastasis
- Serum amylase or pancreatic cancer markers (CA19-9, CEA and a-fetoprotein) are usually normal
- It usually has better prognosis than the typical adenocarcinoma of the pancreas
- It is treated with surgery and complete resection is usually curative
- Ultrasound-large well-defined mass with heterogenous appearance due to its cystic and solid components
- CT scan- well-encapsulated lesion with varying degree of solid and cystic component with hemorrhagic degeneration. Calcification and enhancing solid areas may be present at periphery and cystic portion centrally
- MRI shows pure solid consistency in 80% of cases
Recent Comments