
Case contribution: Dr Radhiana Hassan
Clinical:
- A 46 years old male with chronic sinusitis
- Presented with right frontal swelling and headache
- Blood investigation: Hb=13.4, TWBC= 7.7
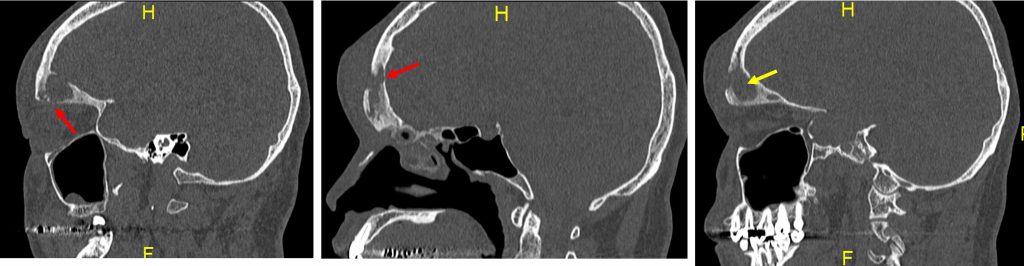
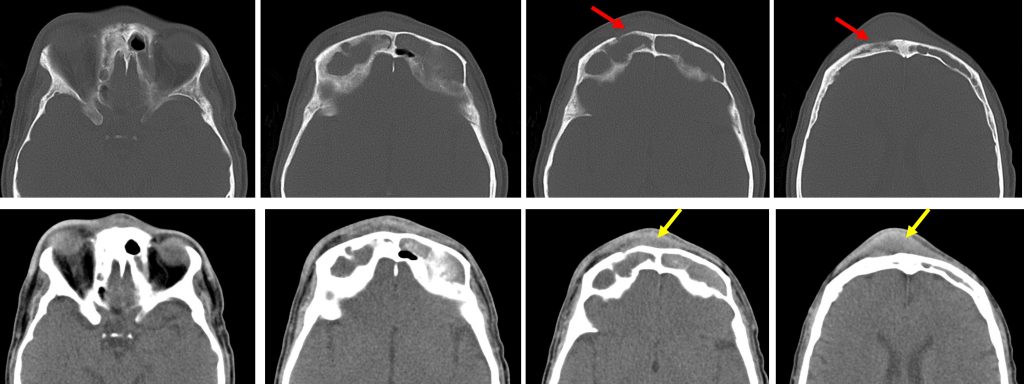
CT scan findings:
- There is expansion with total opacification of both frontal sinuses.
- The sinuses are filled with soft tissue density lesion.
- There is associated intralesional calcification and hyperdense areas within the left frontal sinus.
- This lesion is seen extending anteriorly into the subgaleal region (yellow arrows).
- No calcification or air pockets within.
- There is also soft tissue swelling at right preseptal region.
- The walls of the right frontal sinus, right ethmoidal air cells and medial wall of the right orbit are sclerosed.
- Bony defect at anterior wall of right frontal sinus is also noted (red arrows).
- Subtle lytic destruction is also seen involving posterior wall of right frontal sinus and right lamina papyracea.
- Both cribriform plates and nasal septum are intact.
- No obvious intra orbital or intracranial extension is seen.
Diagnosis: Pott puffy tumour
Progress of patient:
- FESS and open frontal sinus surgery performed.
Discussion:
- It refers to clinical presentation of a frontal mass as a result of osteomyelitis with subperiosteal abscess, most commonly as a complication of frontal sinusitis.
- It is a non-neoplastic condition predominantly affects children and adolescents.
- Children are more susceptible because of anatomic and physiologic changes in the developing frontal sinus.
- It is characterized by subgaleal collection, periosteal abscess and osteomyelitis.
- It is usually related to frontal sinus but sometimes can be secondary to mastoid pathology.
- It has become unusual since the availability of antibiotics.
- The most common organisms are Streptococcus spp., Haemophilus influenza, Staphylococcus spp and Klebsiella sp.
- CT typically demonstrate an opacified frontal sinus with stranding and swelling of the overlying scalp.
- Bone window shows defect of anterior wall of the sinus. Contrast study shows focal abscess and may also show intracranial complication.
- MRI is better to delineate subtle findings such as enhancement of dura mater, extra axial fluid collection and area of cerebritis or cerebral abscess.
- Transcortical spreading can result in severe intracranial and orbital complications. Early detection and treatment are crucial because of these potentially life-threatening complications.
Recent Comments